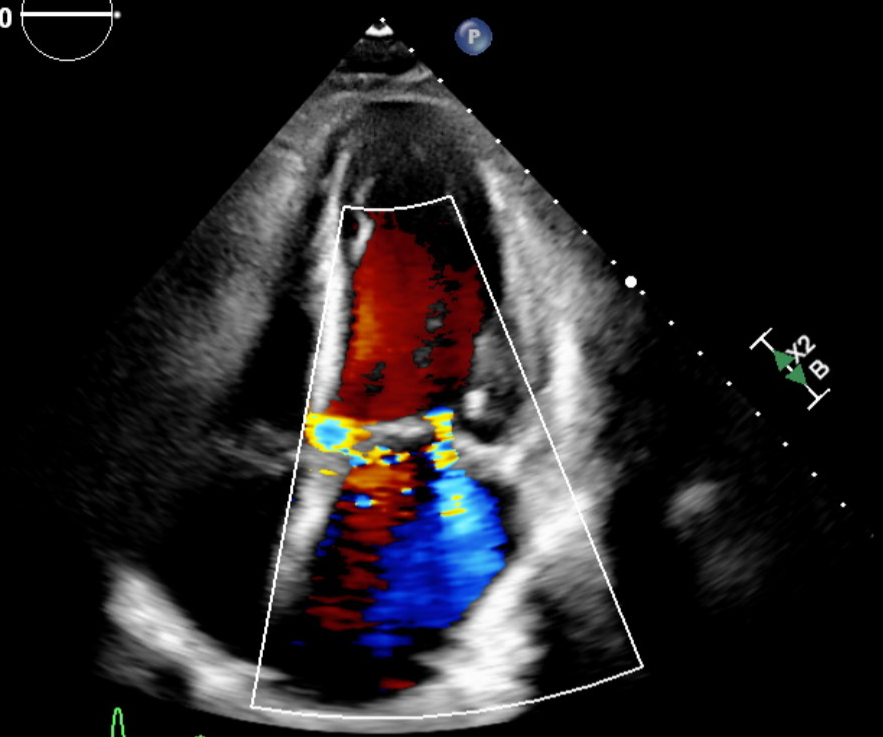
Case Presentation: This case report describes a 63-year-old man with a medical history of hypertension, hyperlipidemia, abdominal aortic aneurysm status post endovascular repair, chronic obstructive pulmonary disease, and alcohol use disorder, who presented to the emergency department with a three-week history of generalized weakness followed by a fever for the last three days. Physical examination revealed scleral icterus, tachycardia, systolic murmur, bibasilar crackles, abdominal distension, and bilateral pitting edema. Laboratory findings showed leukocytosis, macrocytic anemia, metabolic acidosis, elevated brain natriuretic peptide, acute kidney injury, mildly deranged liver enzymes, hyperbilirubinemia, and mild coagulopathy. Computed tomography imaging revealed a cirrhotic liver with sequelae of portal hypertension. The urinalysis was unremarkable. The patient was started on broad-spectrum antibiotics empirically, later tailored to penicillin when blood cultures grew Aerococcus urinae. A transthoracic echocardiogram indicated diastolic dysfunction, aortic and mitral regurgitation, and aortic valve leaflet thickening raising concerns for possible infective endocarditis. While awaiting transesophageal echocardiogram, the patient experienced cardiogenic shock from acute valvular dysfunction with extensive regurgitation unresponsive to vasopressors, ultimately leading to cardiac arrest and death despite resuscitative efforts.
Discussion: Aerococcus urinae is a rare gram-positive coccus that is often misdiagnosed as Staphylococcus, Streptococcus, or Enterococcus. While most commonly implicated in urinary tract infections, Aerococcus urinae infrequently leads to infective endocarditis due to its capacity for biofilm formation and platelet aggregation. Numerous complications have been reported in cases of Aerococcus urinae infective endocarditis, encompassing embolization, valvular dysfunction, stroke, conduction abnormalities, heart failure, and infrequently, valvular ulcer formation, abscess development, pericardial fistula formation, and death. Treatment includes antibiotics and surgical intervention when necessary to prevent these complications.This case underscores the potential severity of Aerococcus urinae infections leading to infective endocarditis and subsequent cardiac complications. Despite the rare nature of this pathogen, its ability to induce acute valvular dysfunction leading to cardiogenic shock and fatal outcomes is evident.
Conclusions: This case report adds to the evolving body of knowledge regarding the clinical spectrum and outcomes associated with Aerococcus urinae infections, emphasizing the need for prompt intervention to mitigate potential life-threatening consequences.