Background: In 2025, CMS implemented a new inpatient quality measure to report on age-friendly care, the 4Ms Framework: what matters, medications, mentation, and mobility. Hospitalization at Home (HaH) provides hospital-level care to patients in the comfort of their own homes. This study assesses whether HaH delivers age-friendly care aligned with the 4Ms Framework.
Methods: We performed a retrospective review of 140 patients admitted to our institution’s HaH service from January–August 2025. Patients were included if they were ≥65 years old and admitted while physically located in the Emergency Department. Clinical documentation was reviewed for the presence of 4Ms-aligned elements. -What Matters: goals-of-care discussions, healthcare proxy/surrogate identification, caregiver involvement, MOLST documentation, code status. -Medications: medication reconciliation completion, unintended discrepancies, high-risk discrepancies. -Mentation: mental status examination, presence of dementia, documented delirium. -Mobility: functional assessments, PT/OT involvement, durable medical equipment (DME) usage.
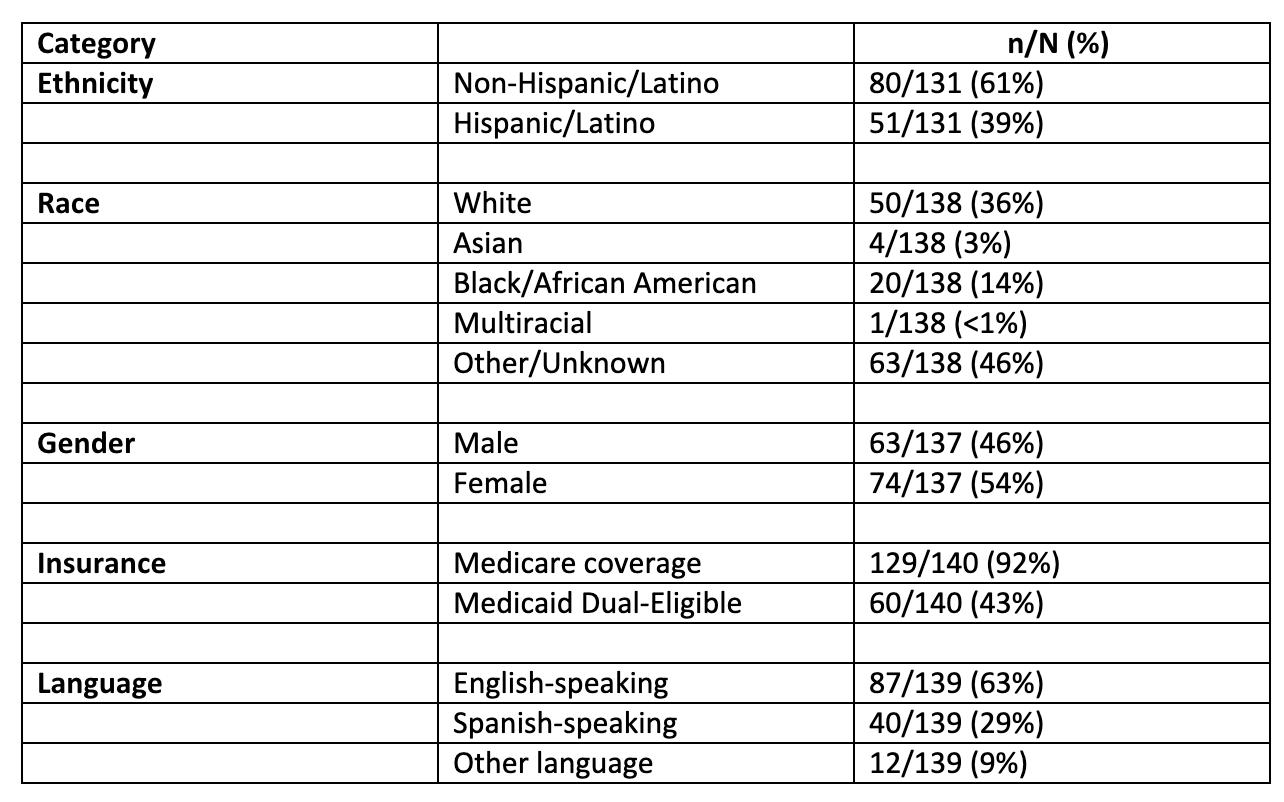
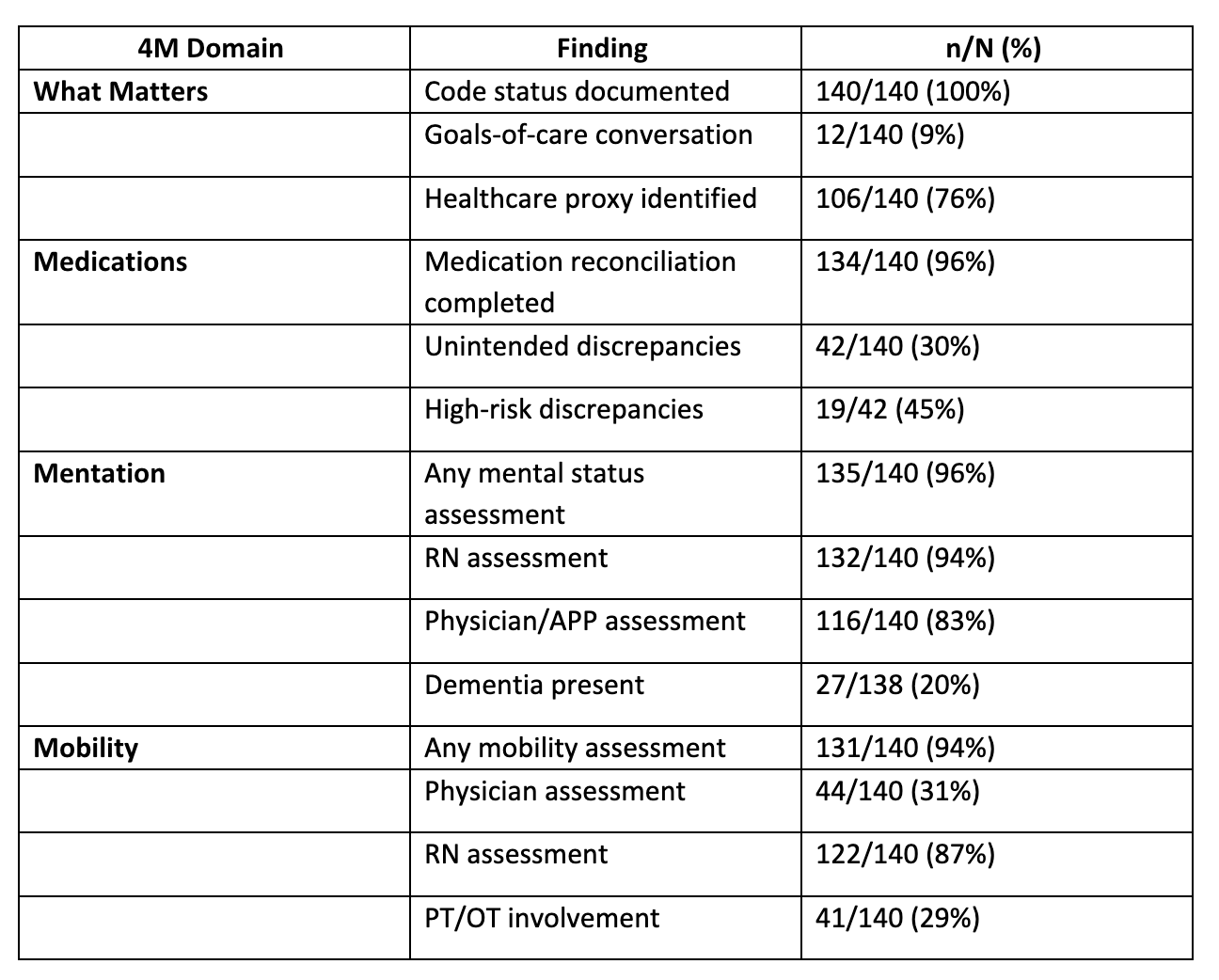
Results: Among the 140 patients reviewed, ethnicity was reported for 131 patients: non-Hispanic/Latino (61%) and Hispanic/Latino (39%). Race was reported for 138 patients: White (36%), Asian (3%), Black/African American (14%), multiracial (< 1%), and other/unknown (46%). Of 137 patients reporting gender, 63 were male (46%) and 74 female (54%). When combining primary and secondary insurance, 92% had Medicare coverage and 43% had dual Medicaid coverage. Preferred language was documented for 139 patients: English (63%), Spanish (29%), and Other (9%).Matters Most: 100% of patients had code status documented, 9% of patients had separate goals of care discussion documented while on service. 76% had healthcare proxy or surrogate identified. Medications: Medication reconciliation was completed in 96% of cases, with unintended discrepancies identified in 30% of cases. A total of 19 of the 42 unintended discrepancies were identified as high-risk medications. Mentation: A mental status assessment was completed for 96% of cases, by an RN in 94% and a physician or APP in 83% of cases. Dementia was present in 20% of cases.Mobility: Mobility assessments were performed for 94% of cases, by physicians or APP in 31% and by an RN in 87% of cases. PT/OT evaluated 29% of cases.
Conclusions: Our findings demonstrate that HaH consistently incorporated core elements of age-friendly care across all 4M domains, establishing it as an age-friendly alternative to traditional inpatient hospitalization. The home-based nature of HaH care, delivered in patients’ usual environment, inherently enables care teams to integrate patients’ goals, home circumstances, and support systems into tailored interventions. However, this model’s reach remains limited, serving approximately 15% of the inpatient population. This disparity underscores a critical need: while HaH excels at delivering age-friendly care, the majority of hospitalized older adults cannot access these benefits. Future research must prioritize identifying the specific HaH care delivery elements that drive age-friendliness and developing strategies for translation into traditional hospital settings. By adapting HaH’s successful components for brick-and-mortar facilities, we can expand age-friendly care to traditional hospitalization, ensuring equitable access to person-centered geriatric care across all care settings.