Background: Patients with liver disease have complex hemostatic abnormalities that can cause severe hematologic complications. Although they are known to be at increased risk for bleeding, newer evidence has dispelled the notion that they are protected from venous thromboembolism (VTE). Liver disease is also associated with multiple complications, such as varices, ascites, and hepatic encephalopathy, and laboratory derangements, including thrombocytopenia and elevated INR. However, the effect of these complications on VTE development remains unclear, as prior studies have shown variable results. We conducted a retrospective analysis to identify risk factors for VTE among patients with liver disease.
Methods: Patients with liver disease and VTE admitted to hospitals within a large suburban health system from 2015 to 2025 were enrolled in this case-control study and compared with those with liver disease but no VTE. Patients were at least 18 years old at the time of admission. Those with anticoagulant use prior to admission or known coagulopathy were excluded. A total of 1,285 patients were included. Demographics, past medical history, admission diagnoses and complications, medication use, and laboratory values were analyzed using the chi-square test or Fisher’s exact test for categorical variables and the two sample t-test or Mann-Whitney test for continuous data to identify the presence of risk factors for VTE. Data were presented as mean ± standard deviation, median [25th, 75th percentiles], or frequency and percent. Results were significant at p< 0.05 and analyses were performed using SAS v9.4.
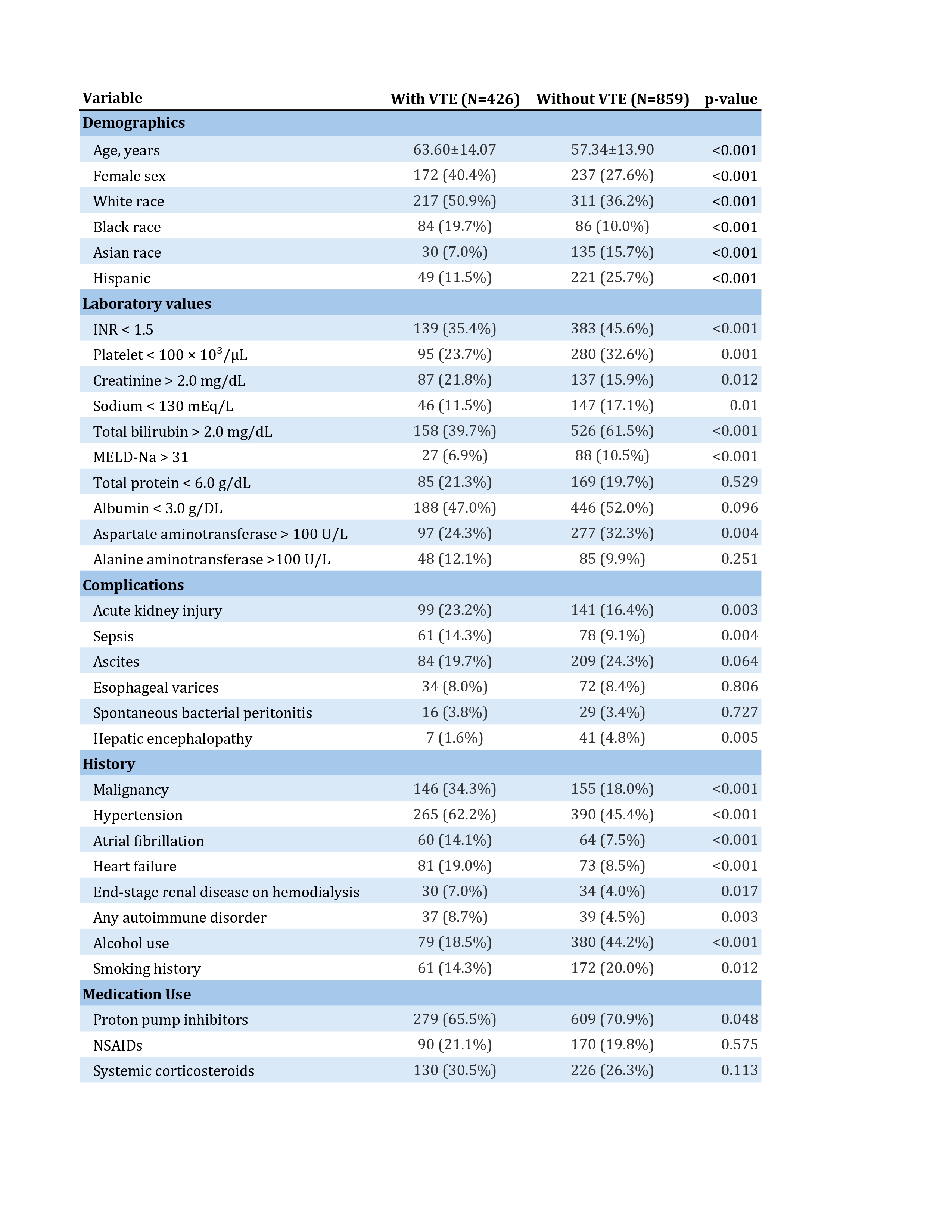
Results: Of the 1,285 patients included, 426 (33.2%) had VTE and 859 (66.8%) did not. Compared with controls, patients with VTE were older and more likely to be female; the racial and ethnic distributions differed significantly between groups. Those with VTE were less likely to have elevated INR, thrombocytopenia, hyponatremia, hyperbilirubinemia, elevated AST, or MELD-Na >31; conversely, they were more likely to have elevated creatinine. There was no significant difference in total protein, albumin, or ALT. Those with VTE were more likely to have AKI or sepsis and were less likely to have hepatic encephalopathy. Rates of ascites, esophageal varices, and spontaneous bacterial peritonitis did not differ significantly. Malignancy, hypertension, atrial fibrillation, heart failure, end-stage renal disease requiring hemodialysis, and autoimmune disorders were more common in the VTE group; alcohol use and smoking history were more common in the control group. Use of proton pump inhibitors was more frequent in the VTE group, with no significant difference in NSAID or systemic corticosteroid use. Table 1 more precisely describes risk factors. Subjects in the VTE group were more than twice as likely to die as compared to the control group (OR = 2.44; 95% CI: 1.88–3.18).
Conclusions: Although liver disease was previously thought to protect against VTE, newer research has shown that patients with liver disease are at least at similar risk for VTE as those without liver disease. We describe factors more and less commonly associated with VTE among patients with liver disease. Factors typically associated with advanced liver disease or acute liver failure appear to be protective against VTE, while those linked to increased VTE risk in other populations also appear to increase risk among patients with liver disease. VTE in patients with liver disease should be considered in those with stable disease and traditional risk factors.