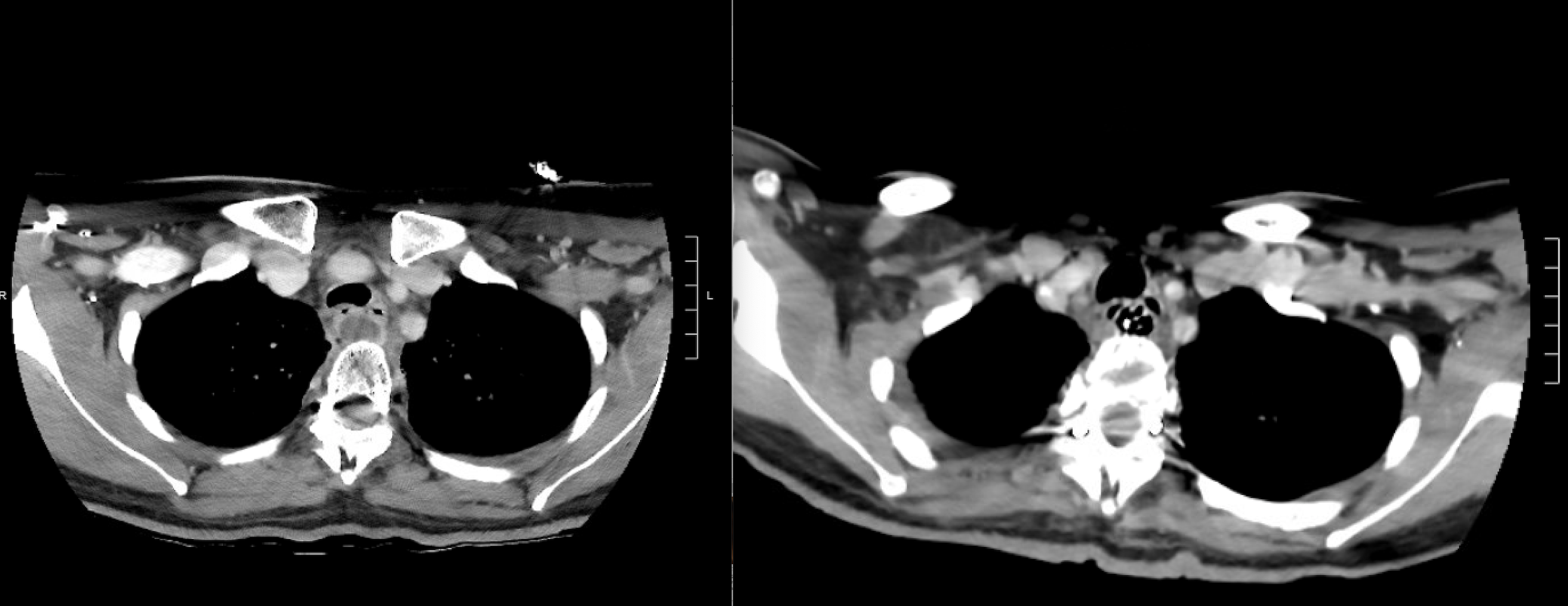
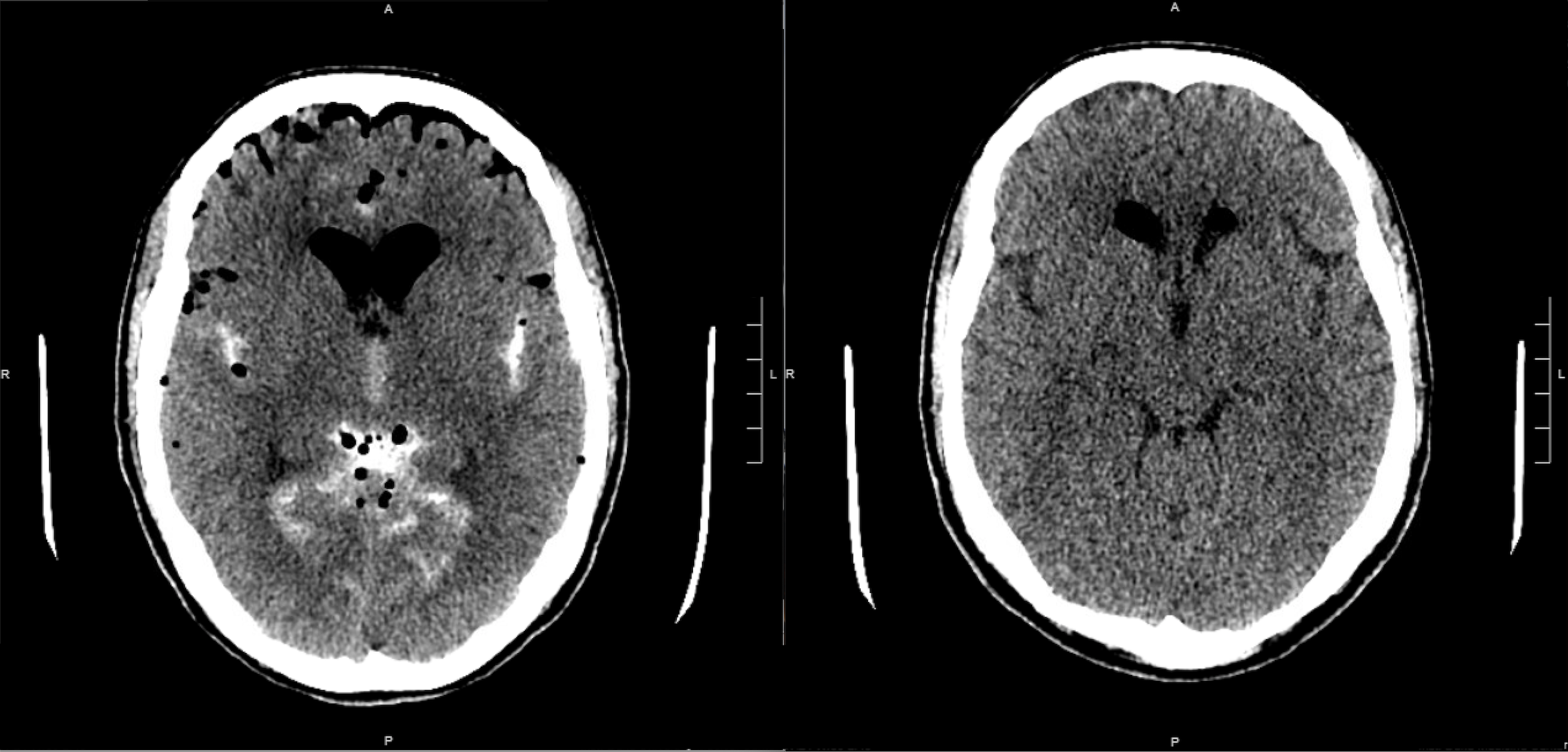
Case Presentation: A 38-year-old woman with a history of epidural giant cell tumor of the cervical spine (diagnosed 15 years prior to admission, in remission after C7-T1 corpectomy and fusion, chemotherapy and radiation) was admitted to the hospital with several months of progressive dysphagia. Endoscopic biopsy of a posterior cervical esophageal lesion demonstrated invasive squamous cell carcinoma. Soon after biopsy she developed a fever and computed tomography (CT) imaging revealed a rim-enhancing fluid collection in the retroesophageal space directly anterior to her spine hardware (Figure 1a). A video-assisted thoracoscopy with placement of a retroesophageal drain was performed (Figure 1b), with operative cultures yielding E. coli. The patient defervesced with drain placement and targeted intravenous antibiotics. Given persistent output ten days after drain placement, a CT of the neck demonstrated small volume pneumocephalus concerning for communication between the retroesophageal space and the spinal canal. Lumbar puncture was performed and CSF cultures grew E. coli. The patient subsequently developed nausea, vomiting, and progressive headache, prompting CT brain which demonstrated significant increase in pneumocephalus (Figure 2a). After multidisciplinary discussion between Hospital Medicine, Neurosurgery, Infectious Disease, and Thoracic Surgery, the consensus was that the indwelling retroesophageal drain might be allowing for communication of air into the subarachnoid space; thus, the decision was made to remove the drain. The patient’s headache improved and CT brain performed four days later demonstrated dramatic reduction in pneumocephalus (Figure 2b), supporting the hypothesis that the drain was responsible for the pneumocephalus. To provide assurance prior to initiation of cancer-directed therapy, a CT Gastrografin study was performed and demonstrated no evidence of esophageal leak. The patient initiated cisplatin and radiation and has since been discharged from the hospital in stable condition without neurologic deficits.
Discussion: Pneumocephalus is when gas is detected within the cranial vault. The most common causes of pneumocephalus are head trauma and surgeries involving the brain, skull, or spine; CNS infections, malignancy, spinal fluid sampling or injections, and positive pressure ventilation (particularly in patients with head trauma or recent skull base surgery) also place patients at risk for pneumocephalus. We present a unique case of pneumocephalus in which the combination of an indwelling surgical drain and a distant spine surgery allowed for introduction of air into the subarachnoid space. Detection of pneumocephalus merits immediate neurosurgical evaluation and monitoring to ensure the patient does not develop tension pneumocephalus, which can be life threatening. Definitive treatment involves addressing the underlying cause of pneumocephalus. In our case, the Hospital Medicine team played a critical role in coordinating care and charting a course of action, which ultimately involved removal of the indwelling drain and complex risk/benefit discussions prior to initiation of cancer-directed therapy.
Conclusions: Pneumocephalus is a rare but serious imaging finding. In hospitalized patients who develop pneumocephalus, iatrogenic causes must be considered, and prompt involvement of surgical specialties is essential. Hospitalists are experts in coordinating complex, multispecialty care, as demonstrated in this case.