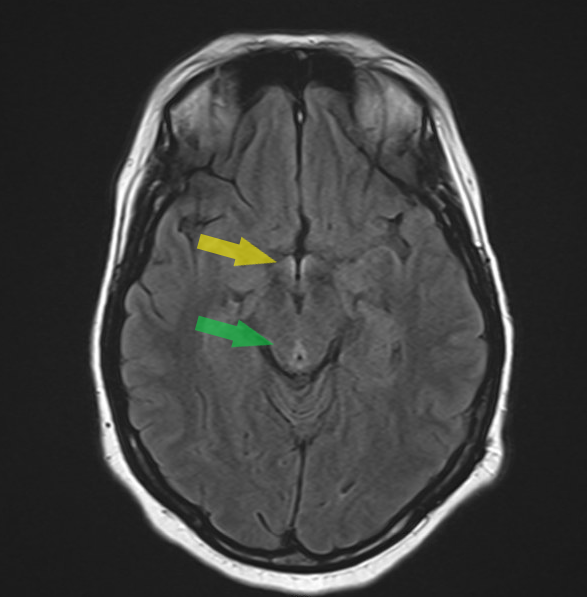
Case Presentation: A 36-year-old female with GERD, H. pylori infection, and cholelithiasis post cholecystectomy was admitted with 1 month of progressive weakness, blurry vision, and pain limiting ambulation. She needed a rollator and assistance for transfers. She had a 60-lb weight loss with anorexia after the recent death of her father. Family noted odd behavior with visual hallucinations; no alcohol or drug abuse.On neurologic exam, she had delayed cognitive processing, bidirectional horizontal nystagmus, decreased visual acuity, sensorimotor hearing loss, bilateral lower extremity weakness, areflexia with hypotonia, gait ataxia, and sensory ataxia. There was length-dependent sensory dysfunction in vibration, proprioception, pinprick, and temperature. Memory and attention were impaired. She remained oriented. Mood was depressed. Ophthalmologic exam found peripapillary white lesions and intraretinal flame hemorrhages.Labs: deficiencies in thiamine (< 20), folate (6.5), vitamin D (< 7) and B12 (116). Lumbar puncture: bland, normal opening pressure. MRI brain: T2 hyperintensity in the periaqueductal gray and hypothalamus, consistent with thiamine deficiency (Figure).The differential for neuropathy with pain and weakness included Guillain-Barre syndrome (ruled out by LP), functional disorder (evaluated by psychiatry due to complicated grief), and vitamin deficiency. The final diagnosis was thiamine deficiency with dry beriberi and Wernicke’s encephalopathy.She was treated with high-dose intravenous thiamine then oral supplementation. Nutrition support included temporary enteral feeds and family collaboration to promote intake. She had gradual improvement in vision, hearing, and strength. Neuropathic pain persisted at discharge to acute rehab.
Discussion: This case highlights the severe neurologic and ophthalmologic manifestations of dry beriberi due to malnutrition triggered by psychosocial stress. Dry beriberi is characterized by peripheral distal axonal neuropathy, sensorimotor deficits, and muscle weakness due to vitamin B1 (thiamine) deficiency. Thiamine is a coenzyme required for aspects of cellular metabolism and initiation of nerve impulse propagation. It may also present with Wernicke’s encephalopathy with ophthalmoplegia, nystagmus, ataxia, and confusion. Typically associated with chronic malnutrition states (ie. alcohol abuse, anorexia nervosa), clinical manifestations of severe thiamine deficiency can be seen after 1-3 months of inadequate intake, as in our case. While functional disorders may be considered in a grieving young woman, organic etiologies must be evaluated first and treated aggressively to restore function and improve symptoms. In patients without overtly apparent malnourishment (normal BMI) or risk factors (alcohol use disorder), the constellation of findings localizing to the peripheral nervous system – sensory ataxia, areflexia, polyneuropathy – with MRI and ophthalmologic changes are classic for thiamine deficiency but may go underrecognized in developed countries.
Conclusions: This case underscores the importance of nutritional assessment in patients with objective and unexplained neurologic symptoms. Thiamine deficiency can present as dry beriberi; hospitalists must maintain suspicion in patients with inadequate intake and multisystem neurologic findings, even in the absence of alcohol use. Early recognition and treatment with aggressive thiamine repletion can prevent irreversible nerve damage and encephalopathy