Case Presentation: A 20-year-old female with no significant past medical history presented to the ED with syncope and fall. She had 5 episodes of syncope without prodrome over the last three months with two occurring in the last two weeks. The patient presented after another syncopal episode resulting in a fall and injury to the right side of her face. On review-of-systems she endorsed frequent self-limiting headaches, but denied fevers, chills, dyspnea, palpitations, chest pain, abdominal pain, nausea or vomiting, diarrhea, dysuria, blood in stool or urine, tremors, diaphoresis, weakness, or hives/allergic reaction. She recalled a mild viral infection 4 months prior. She did not take any medications, had no significant family history, lived an active lifestyle, and denied tobacco, alcohol, and drug use. She was hemodynamically stable while supine with blood pressure (BP) 115/75 mmHg and heart rate (HR) 81 beats/minute (bpm). Active stand test demonstrated BP of 114/70 mmHg and HR of 130 bpm after 5 minutes. Physical exam was notable for sinus tachycardia, normal heart sounds and pulmonary exam, no nystagmus or vision changes, no focal neurologic deficits, faint livedo reticularis in the bilateral legs, and right facial ecchymosis. EKG showed sinus tachycardia at 131 bpm. CBC, CMP, TSH, troponin, BNP, lactate, VBG, and beta-hCG were all normal. Imaging with CTA head/neck and CT cervical spine were negative for vascular abnormalities or traumatic findings. The patient was given 3 x 1L normal saline boluses in the ED without improvement in her orthostatic tachycardia, thus she was admitted for further work-up. Additional testing including morning cortisol level, serum catecholamines, and transthoracic echocardiogram was normal. Postural orthostatic tachycardia syndrome (POTS) was suspected, and the patient was discharged with non-pharmacologic therapies (table 2), two-week ambulatory EKG monitor, outpatient head-up tilt test, and POTS clinic follow-up in 1 month. At her outpatient follow-up, the cardiac monitor recorded intermittent episodes of sinus tachycardiac to 130s during daytime without additional arrhythmias. Tilt table testing confirmed the diagnosis of POTS with pattern suggestive of autonomic neuropathy. The patient remained syncope-free from discharge to 1-month follow-up.
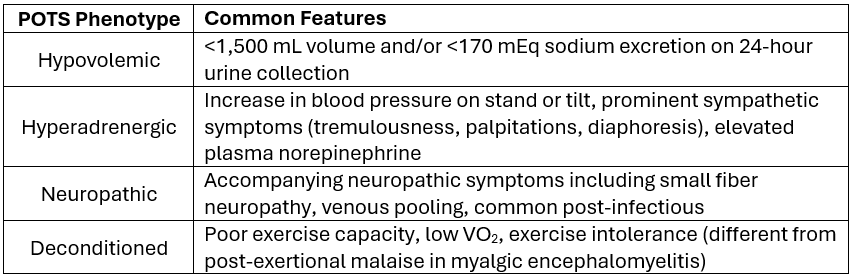
Discussion: This case presents a patient with atypical POTS given frequency of syncope without prodromal symptoms of orthostatic intolerance including nausea, vomiting, lightheadedness, and presyncope. The consensus criteria for diagnosis includes: 1. HR ≥ 30 bpm (≥ 40 bpm if age 12-19 years) within 10 minutes of position change, 2. absence of sustained orthostatic hypotension, 3. frequent symptoms of orthostatic intolerance with rapid improvement upon lying supine, 4. symptoms for ≥ 3 months, and 5. absence of other likely etiology. POTS subtypes and initial management are presented in tables 1 and 2, respectively. Our patient likely had neuropathic POTS and responded appropriately to the recommended interventions.
Conclusions: POTS is a chronic, multisystem disorder with the hallmark feature of postural tachycardia. With increasing prevalence due to the recent COVID-19 pandemic as a viral trigger, it is essential for hospitalists to be aware of POTS, its diagnostic features, and initial management strategies that can be implemented in the acute care setting to reduce recurrent ED visits/hospitalizations and improve patients’ quality of life.