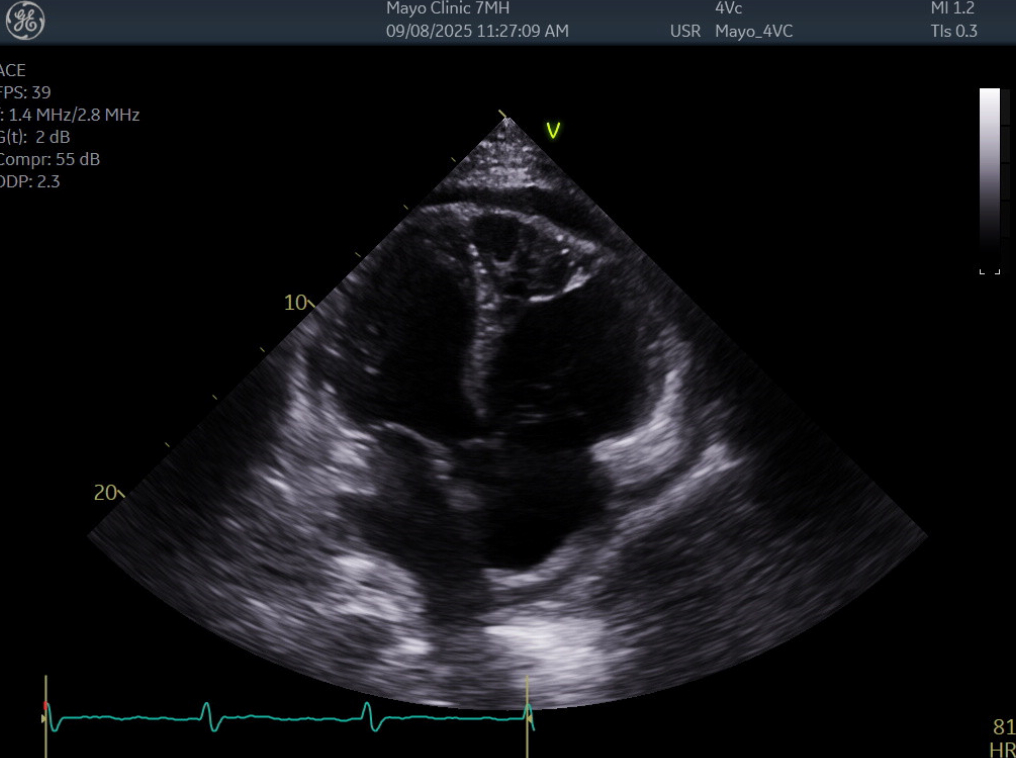
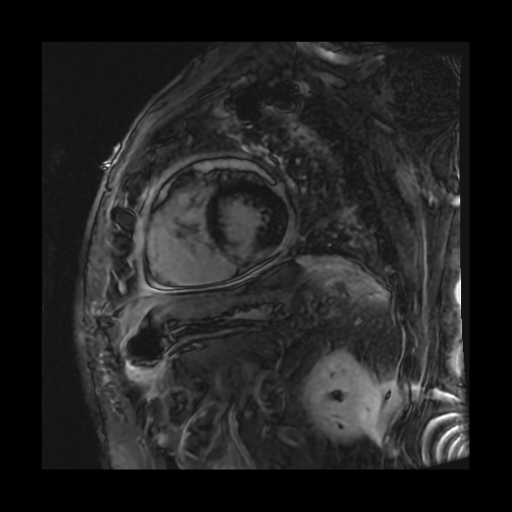
Case Presentation: A 62-year-old male presented to the emergency department with 4-5 days of dizziness, chest pain, and a cough, found to be hypotensive at 75/59. His past medical history was pertinent for hypertension, multiple strokes, tobacco use disorder, and a motorcycle accident in 2024 with extensive injuries, including a traumatic brain injury.On admission, the patient was afebrile and breathing comfortably on room air. He described the chest pain as sharp, persistent, and mild at rest, but worse with inspiration. He reported a dry cough at baseline, but felt it had worsened recently. Physical exam was pertinent for muffled heart sounds, clear lungs, no JVD, and no lower extremity edema. He had no known sick contacts. Initial troponins were mildly elevated at 37 with 2-hour reflex troponin down trending to 28. His EKG had T-wave abnormalities concerning inferior ischemia. Labs showed an elevated CRP at 237, a slight leukocytosis at 11.6, and a negative viral panel. A CT Chest Angiogram was significant for a new moderate right pericardial effusion. An urgent bedside transthoracic echocardiogram (TTE) demonstrated a mild, circumferential pericardial effusion with reduced ejection fracture of 56%, a severely enlarged right ventricle, and a/dyskinesis in the right ventricle. These findings were new from his last TTE in 7/2024. The decision was made to forgo a pericardiocentesis as his overall picture was not consistent with cardiac tamponade. Cardiology recommended a cardiac MRI due to concern for myocarditis and initiating treatment for pericarditis with colchicine and Aspirin. The cardiac MRI showed no evidence of myocarditis, but found transmural enhancements of the left ventricle septum and the right ventricular wall. These findings raised concern for ischemia with possible Dressler Syndrome due to a silent right ventricle infarction. The patient was an overall poor historian, but did say he had some recent chest pain and chose not to seek medical care. The patient’s hypotension improved with fluids and he was eventually discharged on the colchicine and aspirin with close follow-up in the cardiovascular clinic to investigate his new right heart dilation and a/dyskinesia.
Discussion: Dressler Syndrome, also known as Post Myocardial Infarction Syndrome, is a cardiac inflammatory condition that can occur anywhere from 2-6 weeks after a myocardial infarction. Typical presentation includes chest pain, pericarditis, pericardial effusions, and pleuritis. The mechanism for Dressler Syndrome is not entirely understood, but is attributed to be an autoimmune response due to antigens released from damaged myocardial cells. As reperfusion during/after myocardial infarcts has greatly improved, Dressler Syndrome has become far less common. This is credited to a decrease in overall infarct size with a decrease in the body’s exposure to myocardial antigens.
Conclusions: Dressler Syndrome is now most commonly seen after large, silent infarctions, particularly inferior infarctions with right ventricular involvement, such as what we believe happened in this patient. In the end, we believe this case represents the new “classic” presentation of Dressler syndrome from an untreated myocardial infarct. This is supported by the patient’s worsened structural heart disease, EKG findings, cardiac MRI imaging, and clinical presentation.