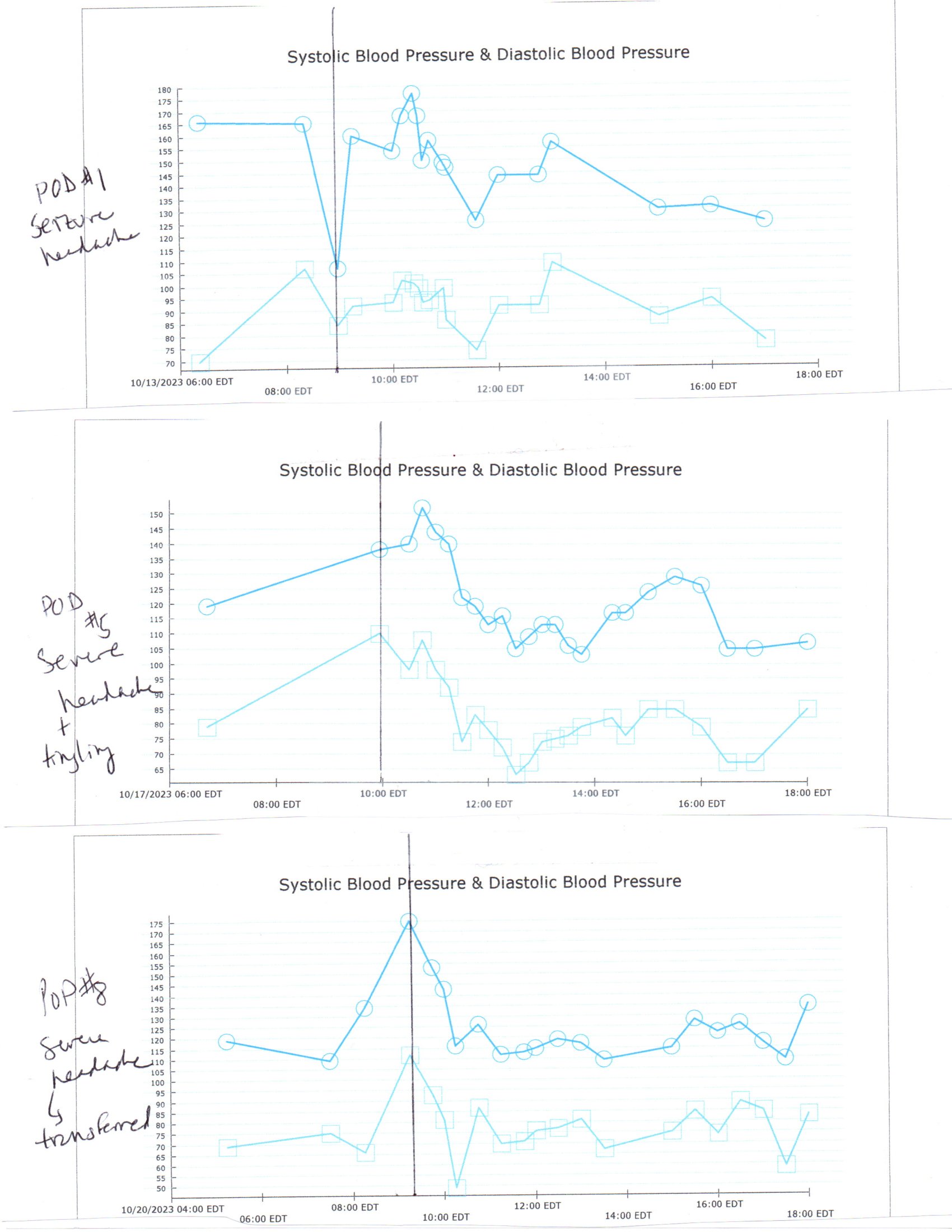
Case Presentation: 34 yo female nonsmoker with PCOS and hirsutism on spironolactone admitted for sleeve gastrectomy for obesity. Pre-op bp 117/50. BP began to increase intraoperatively and postoperatively into the evening with a maximum bp of 181/104. She experienced intractable post-op emesis. After the surgery, she noted chest pain, shaking and numbness in her hands which resolved by the morning. On post-op day 1, BP was 140/92 and she felt “terrible”, with altered cognition, visual deficits, mild left neglect, and severe headache. Soon afterwards, she developed facial twitching, fixed left gaze and rhythmic head turning. MRI findings were consistent with PRES. Labs showed Na+ 127, K+ 3.4, WBC 19K, plt slightly elevated, normal renal function, thyroid function and antibodies normal, SPEP normal, CRP 2.2 (normal < 1.0) PO4 1.8, replaced. Symptoms improved and were thought to be secondary to post-op hypertension and emesis. She remained normotensive for the most part on a simple antihypertensive regimen. However, on post-op day 5, BP increased, and she complained of a severe headache; repeat CT showed cerebral venous sinus thrombosis. IV heparin was initiated, and this diagnosis was favored over PRES at the time. Coagulopathy /autoimmune work up including ANA, AT 3 activity, APC resistance, F5 Leiden, prothrombin, homocysteine, complements and PLA2RAb were ultimately normal. On post-op day 8, she again had a severe headache with hypertension and was transferred to an outside hospital with subsequent discharge on post-op day 13 with a discharge diagnosis of PRES with CVST ruled out as a diagnosis. One month post-op, her neurologist discontinued verapamil as she was orthostatic even on a low dose. Two weeks later she followed up with her surgeon and stated that she was in the midst of a workup for recurrent syncope with her PCP. Her antihypertensive, anticoagulant, and antiepileptic medications had been discontinued without incident.
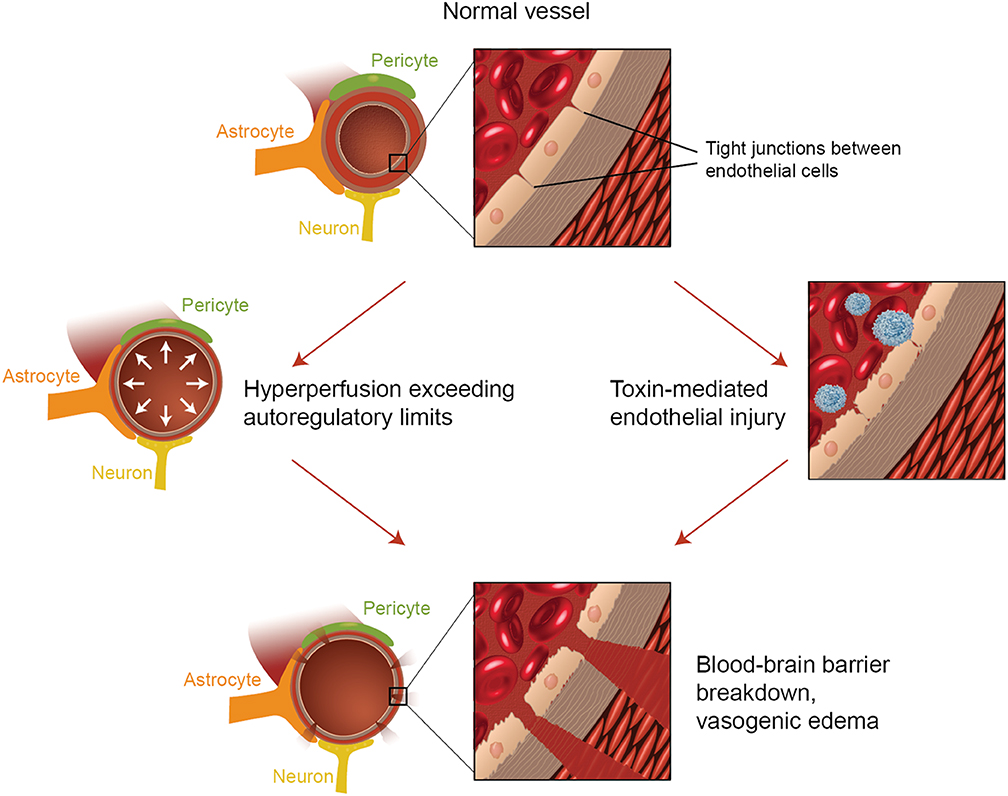
Discussion: Two theories regarding the pathophysiology of PRES are the hypertensive dysregulation theory and the cytotoxic theory. Autoregulation is disrupted at a mean arterial pressure of 150-160 and irreversible brain damage may be seen at systolic blood pressures over 200 (1). Cerebral hyperperfusion overwhelms the brain’s autoregulating capacity, causing dysfunction of the blood brain barrier with subsequent vascular leakage and vasogenic edema.(2,3)Cytotoxic injury causes endothelial dysfunction with vascular leakage and resulting vasogenic edema. In fact, cytotoxic and hypertensive injuries may be caused by different CNS insults but both result in vasogenic edema, a hallmark of the syndrome. In this patient’s case, there was a clear hypertensive component despite no PMH of hypertension. She had stopped spironolactone prior to surgery and this predisposed her to hypokalemia and hypertension. She may have had undiagnosed hypertension. Regarding the possibility of an inflammatory contribution to the PRES, obesity and PCOS have both been implicated causing low-level chronic inflammation. Her CRP was mildly elevated, her white count and platelets were elevated and obesity itself can cause a chronic low -level inflammation.
Conclusions: This patient’s case was unusual in that she had two major setbacks after the initial diagnosis of PRES, illustrating that while PRES is usually a reversible process, recovery does not necessarily occur in a linear fashion. Blood pressure stability and reduction of inflammation is the best way to avoid adverse outcomes.