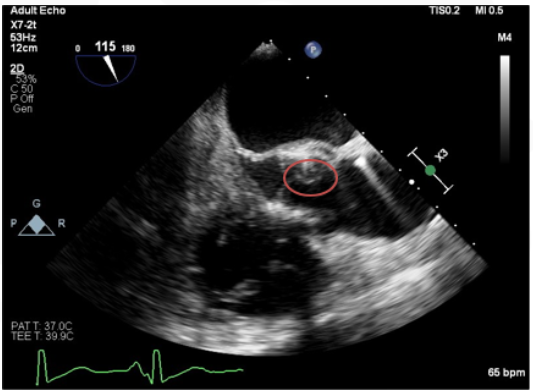
Case Presentation: An 80-year-old Caucasian male with a recent history of transaortic valve replacement three months ago was admitted to the hospital with a history of malaise, and 20 pounds of weight loss in 2 months—no history of diarrhea, fever, vomiting or skin rash. Notably, the patient had multiple admissions for septicemia with salmonella species for which he was treated. On examination, the patient appeared cachectic, but vitals and physical examination, including cardiovascular examination, were within normal limits. Although most of his laboratory values were benign, demonstrating no white count anomalies, and normal renal functions, his blood cultures grew gram-negative rods. Owing to his recurrent salmonella infections and recent valve replacement, a high possibility for infective endocarditis was considered, and he was started on empiric ceftriaxone while awaiting final sensitivities. Subsequent transesophageal ECHO confirmed presence of a vegetation of the non-native aortic valve, and blood cultures grew Salmonella spp. sensitive to ceftriaxone. During his entire stay, his white cell count remained normal. The clinical course was favorable, using an antibiotic regimen of ceftriaxone for six weeks.
Discussion: Salmonella endocarditis is a rare diagnosis, and the absence of ‘classic’ Salmonella symptoms like fever, diarrhea, skin rash ‘rose spots,’ bradycardia and neither leukocytosis nor leukopenia makes this patient’s presentation more unique. A large 16-study case series details how uncommon Salmonella endocarditis is, accounting for less than 0.01% of total bacterial endocarditis cases, with the majority affecting the mitral valves. However, the common theme of presenting symptoms seemed to be fever and diarrhea, among others. Hence, it is vital to have a high degree of suspicion, especially in a predisposed patient such as this gentleman with a valve replacement and multiple comorbidities, with the additional history of Salmonella bacteremia and treat accordingly to prevent the mortality and morbidity that ensues. Although Salmonella prosthetic valve endocarditis is considered an indication for surgical replacement of the prosthesis, this case indicates that prolonged treatment with antibiotics may be an alternative, provided the patient is hemodynamically stable.
Conclusions: In conclusion, this case underscores the rarity and atypical presentation of Salmonella endocarditis, emphasizing the importance of maintaining a high index of suspicion in predisposed patients. The findings suggest that prolonged antibiotic therapy can be a viable alternative to surgical intervention in stable patients with Salmonella prosthetic valve endocarditis, offering a potentially less invasive treatment option.