Case Presentation:
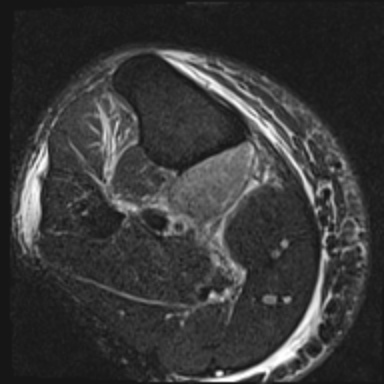
A 47 year-old African American male presented with lower extremity pain and swelling. Three weeks prior he started azilsartan/chlorthalidone for hypertension. A week later, pain and swelling of his right leg began, worsening with ambulation. He denied trauma or unusual physical exertion. Review of symptoms elicited a history of chronic bilateral leg cramps. Physical exam revealed an obese gentleman in obvious discomfort. The right lower extremity was tense and tender with increased circumference compared to the left. Weight-bearing intensified the pain. Doppler ultrasound was negative for DVT. All initial laboratory studies were normal except for an increased creatine kinase of 438U/L. The pain worsened and serial evaluations revealed a warm leg with paresthesias, increasing tightness, inability to plantar or dorsiflex the ankle, and intact pedal pulses. The CK level peaked at 3,168U/L while inflammatory markers were elevated: CRP 6.5, ESR 28. Compartmental pressures were normal on serial testing. MRI defined a focal myositis involving the popliteal muscle. Given his history of muscle cramps and evidence of acute muscle injury, vitamin D deficiency was suspected and confirmed by PTH and vitamin D levels of 60ng/L and 12pg/mL, respectively. On day three of admission, prednisone and vitamin D were started for a working diagnosis of inflammatory myositis induced by an ARB in the setting of vitamin D deficiency. A day after prednisone was started, symptoms improved and his CK trended down. By hospital day 7, the patient reported less pain, had an improved exam, and CK decreased to 576U/L. Vitamin D was continued with a two week course of prednisone. At outpatient follow up he reported near complete recovery of his pain as well as resolution of his muscle cramps.
Discussion:
Extraskeletal manifestations of vitamin D deficiency are gaining recognition. Muscle cramps are a common complaint of vitamin D deficiency but case reports of myositis due to vitamin D deficiency are sparse and related mostly in combination with statins. ARB’s are commonly used anti-hypertensives with muscle spasms as a potential side effect. High compartmental pressures in a limb impair neurovascular integrity, and damage may result if not recognized and managed quickly and appropriately. This is a case of focal myositis with early signs of compartment syndrome believed to be induced by the initiation of an ARB in the setting of vitamin D deficiency. With recognition of an underlying etiology, appropriate medical management prevented worsening of muscle damage and a potential surgical procedure.
In patients who develop rhabdomyolysis or a focal myositis after initiation of an ARB, consider vitamin D deficiency as a contributing factor. It is not known if correction of the vitamin D deficiency allows for later use of such anti-hypertensive agents.