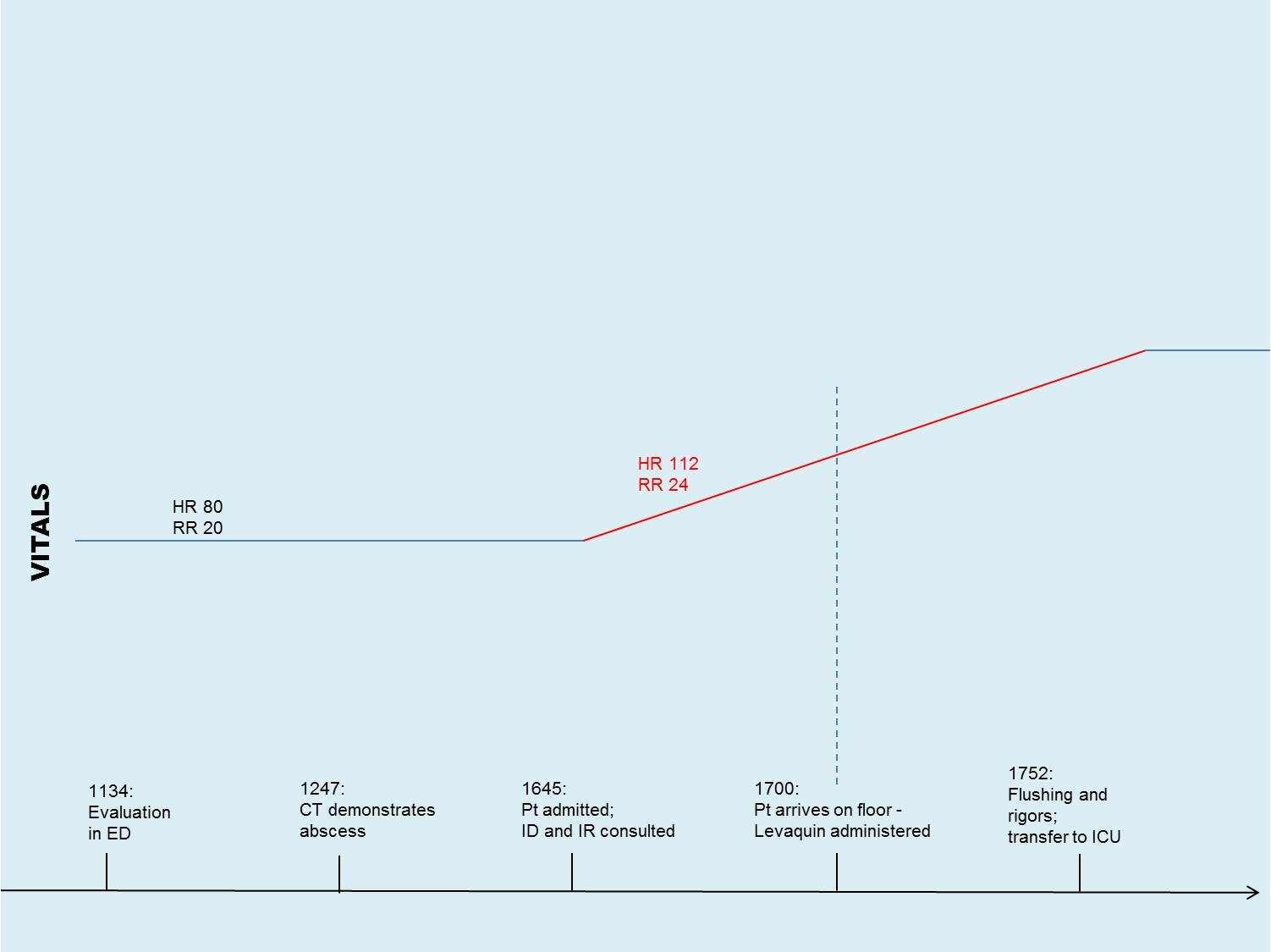
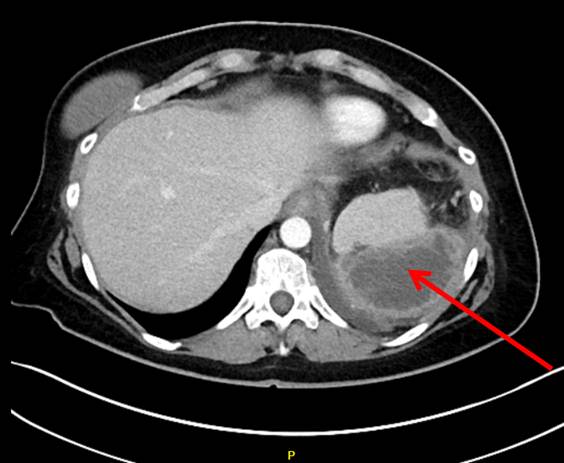
Case Presentation: A 54-year old female was hospitalized for 3-week history of abdominal pain, chills, nausea and diarrhea. Her past medical history was significant for multiple self-reported antibiotic allergies, Roux-en-Y gastric bypass complicated by gastrojejunostomy leak, and prior perisplenic abscess requiring percutaneous drainage. On admission, blood pressure was 137/79, heart rate of 80, respirations 20, saturating at 98% on room air. Physical exam revealed periumbilical tenderness without guarding or rebound. Laboratory workup revealed leukocytosis of 20.4 x10(9)/L. Computed Tomography (CT) abdomen/pelvis demonstrated re-accumulation of a loculated 7.8 x 4.9 cm perisplenic fluid collection. Patient was started on Levaquin and Metronidazole for intraabdominal abscess. Within minutes of receiving Levaquin, the patient experienced acute flushing, rigors and rapid shallow breathing with desaturations into the low 80s suspicious for anaphylaxis, but remained normotensive. Levaquin was stopped and replaced with Aztreonam, and patient was treated appropriately for allergic reaction. Percutaneous drain was placed for perisplenic abscess. Patient responded well to treatment. Blood cultures revealed no growth, but drain cultures grew Pseudopropionibacterium propionicum. Patient’s history of antibiotic allergies was without clear evidence of allergy to Levaquin, therefore a graded Levoquin challenge test was performed during hospitalization. On day 3, patient successfully completed the graded Levaquin challenge with no reaction. Patient was discharged to home 2 days later on oral Levaquin with outpatient follow-up.
Discussion: This case demonstrates the challenge of managing patients with self-reported allergies to multiple antibiotics. These patients often require intravenous antibiotics on discharge, which are associated with their own complications and high cost. Fluoroquinolone hypersensitivity reactions are rare, particularly in comparison to other antimicrobials such as beta-lactams, with reported incidences ranging from 1-44 per 100000. The role of skin testing for fluoroquinolone tolerance is limited as it remains unvalidated, cannot distinguish between IgE and non-IgE mediated reactions and is contraindicated in recent episodes of anaphylaxis due to fluoroquinolones. Patients with hypersensitivity reactions less severe than anaphylaxis, such as flushing, urticaria or rash likely benefit from a graded challenge.
Conclusions: For patients with multiple self-reported antibiotic allergies, graded challenge of antibiotic is an alternative. If successful, it is a safe and cost-effective way to treat infection. Accurate and appropriate documentation of patient allergic history reduces overuse of and inappropriate administration of broad spectrum antibiotic therapy.