Background: Diagnostic consultations between the General Internal Medicine (GIM) departments and specialty departments are becoming increasingly important to achieve team-based diagnosis and diagnostic excellence, but there have been limited studies on the appropriateness of the GIM diagnostic consultations with specialty departments. We conducted this study to clarify the appropriateness of diagnostic consultations from the GIM department to specialty departments, and the factors contributing to the inappropriateness.
Methods: This was a single-center, retrospective, observational study conducted at a university hospital in Japan. Consultations from the GIM department to other specialty departments for outpatients and inpatients aged 20 years and older between January 1, 2021, and December 31, 2021, were included. Data were extracted from electronic medical records. The purpose of the consultation was classified into diagnostic consultations (definitive diagnosis or undetermined diagnosis) and other. Among the consultations for definitive diagnosis, where the name of the new diagnosis was included in the GIM department’s consultation letter, and among the consultations for undetermined diagnosis, those resulted in new diagnoses at the initial specialty department were classified as appropriate diagnostic consultations. The primary outcome was the proportion of appropriate diagnostic consultations. Secondary outcomes were the breakdown and proportion of consultation purposes from the GIM department to the specialty department, and the factors associated with inappropriate diagnostic consultations.
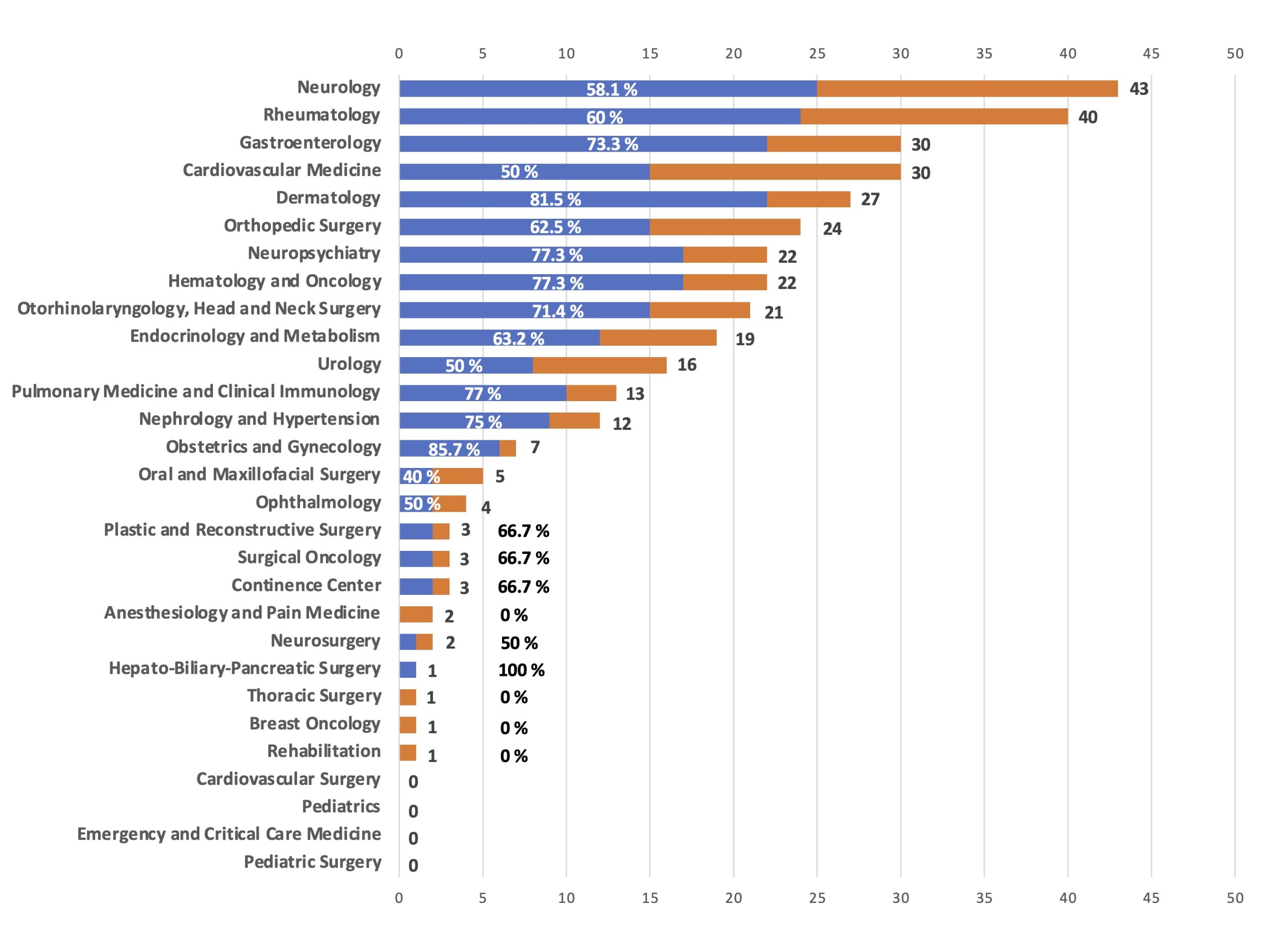
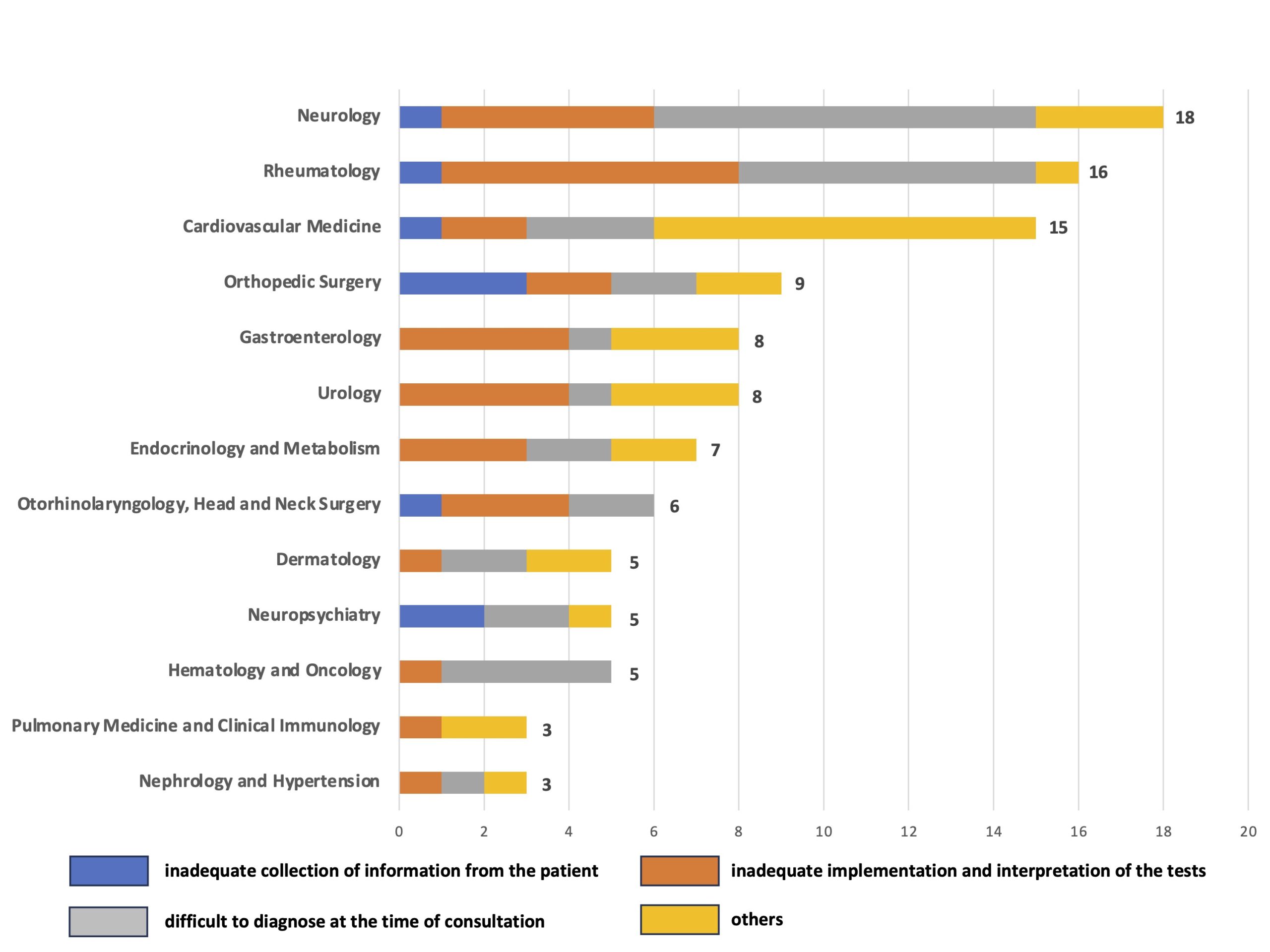
Results: A total of 610 consultations on 454 patients were included. Diagnostic consultations comprised 352 cases out of 610 (57.7%), including 116 cases (19.0%) for definitive diagnosis and 236 cases (38.7%) for undetermined diagnosis. Of the 352 diagnostic consultations, 229 cases (65.1%; 95% CI, 59.9-69.9) were determined to be appropriate. The top five specialty departments to which the GIM department made diagnostic consultations were neurology, rheumatology, gastroenterology, cardiovascular medicine, and dermatology (Image 1). Factors contributing to inappropriate diagnostic consultations included difficult to diagnose at the time of consultation due to undifferentiated symptoms and findings in 41 cases (33.3%), inadequate implementation and interpretation of the tests in 39 cases (31.7%), inadequate collection of information from the patient in 12 cases (9.8%), and other in 31 cases (25.2%) (Image 2).
Conclusions: Diagnostic consultations accounted for approximately 60% of all consultations from the GIM department to specialty departments within a university hospital, in which 30% were inappropriate. The main factors contributing to inappropriate diagnostic consultations were non-specific undifferentiated conditions and inappropriate implementation and interpretation of diagnostic tests.