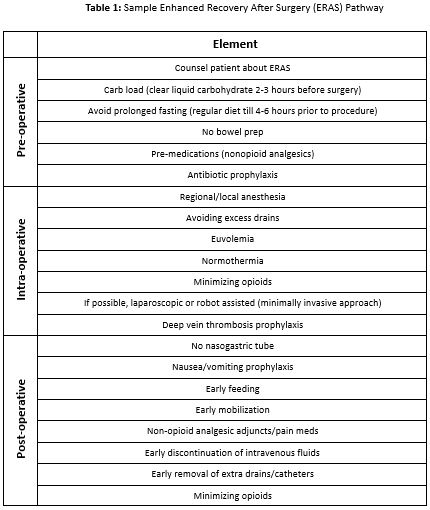
Background: Enhanced Recovery After Surgery (ERAS) is a framework or pathway of standardized preoperative, intraoperative, and postoperative elements shown to improve recovery after a surgical operation (Table 1). ERAS has shown benefits in pediatrics by reducing hospital length of stay, opioid use, readmission rates, health care costs and improving patient satisfaction scores(1,2). At our institution, only a few pediatric surgical subspecialties consistently use ERAS. As hospitalists, we aim to collaborate with surgeons to implement ERAS for our shared patients on the surgical co-management inpatient team, and this survey is a first step towards achieving that goal. Our goal with this survey was to assess pediatric surgeons’ perceptions of ERAS implementation and standardization for perioperative patients at a tertiary, academic children’s hospital.
Methods: An inter-disciplinary team of hospitalists, surgeons, and a survey methodologist created a de-novo, 35-question survey. The questions were refined to achieve the intended effect via cognitive interviews. A REDCap(3) survey link was emailed to all pediatric surgical providers, including advanced practice providers, trainees, and attendings. The survey remained open for 48 days from April to June in 2024 with four follow-up reminders sent every ten days to non-responding surgical providers. Data were analyzed descriptively using frequencies and percentages.
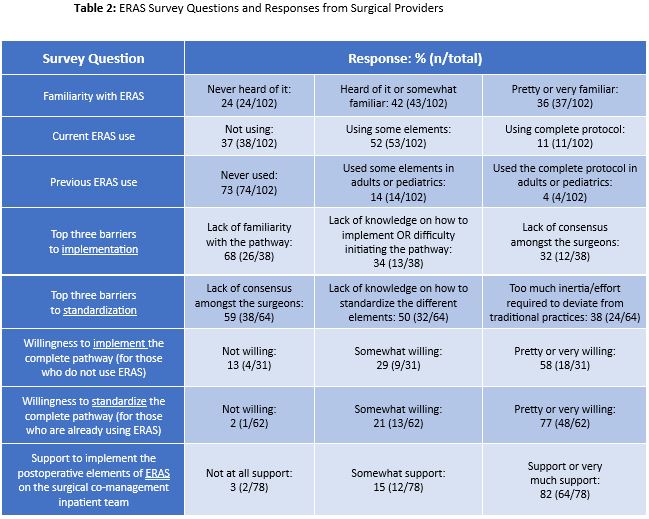
Results: We received 102 out of 345 possible responses (30%). Respondents were mostly orthopedic (23%) and general pediatric surgeons (23%). Nearly half were attendings (43%) and 34% were advanced practice providers. The main survey results are summarized in Table 2. Most (82%) support or very much support implementing postoperative ERAS on the surgical co-management team, but familiarity with ERAS varied, with 24% having never heard of ERAS. This lack of familiarity (68%) and knowledge on how to implement (34%) were the main barriers for ERAS implementation. Barriers for standardization included lack of consensus amongst the surgeons (59%) and a lack of knowledge on how to standardize (50%). Only 11% reported using all of ERAS currently, 52% using some elements, and 37% not using ERAS at all. 73% had not used ERAS prior to their current role. 58% were pretty or very willing to implement the complete ERAS pathway and 77%, amongst those who were already using ERAS, were pretty or very willing to standardize the complete pathway for all surgical patients at our children’ hospital.
Conclusions: Most surgeons are in favor of implementing and standardizing the ERAS pathway, especially for their patients on the surgical co-management team. However, most surgical providers are not very familiar with ERAS which is a key barrier to its implementation. These data will guide us in collaborating with various surgical subspecialties to implement the ERAS pathway for their patients to improve patient care outcomes and reduce associated health care costs.