Background: In a technology-driven era, it is no surprise that the majority of learners prefer multimodal resources when learning new material. Patient discharge education is no exception to this, and several studies have demonstrated that providing digital discharge education (DDE) can help with patient comprehension, information retention, and patient self-efficacy with medication (1, 2, 3). Additionally, several studies show that patients prefer video-based education (2). Pediatric-based studies on DDE are limited in number as advances in multimodal patient education are still ongoing, including at our hospital, where the primary method of discharge education involves printed written material. This study aims to increase the percentage of caregivers of hospitalized patients on the Pediatric Hospital Medicine (PHM) service with primary hospital diagnoses of bronchiolitis, asthma, or seizures who access DDE that were sent it from 0% to 25%.
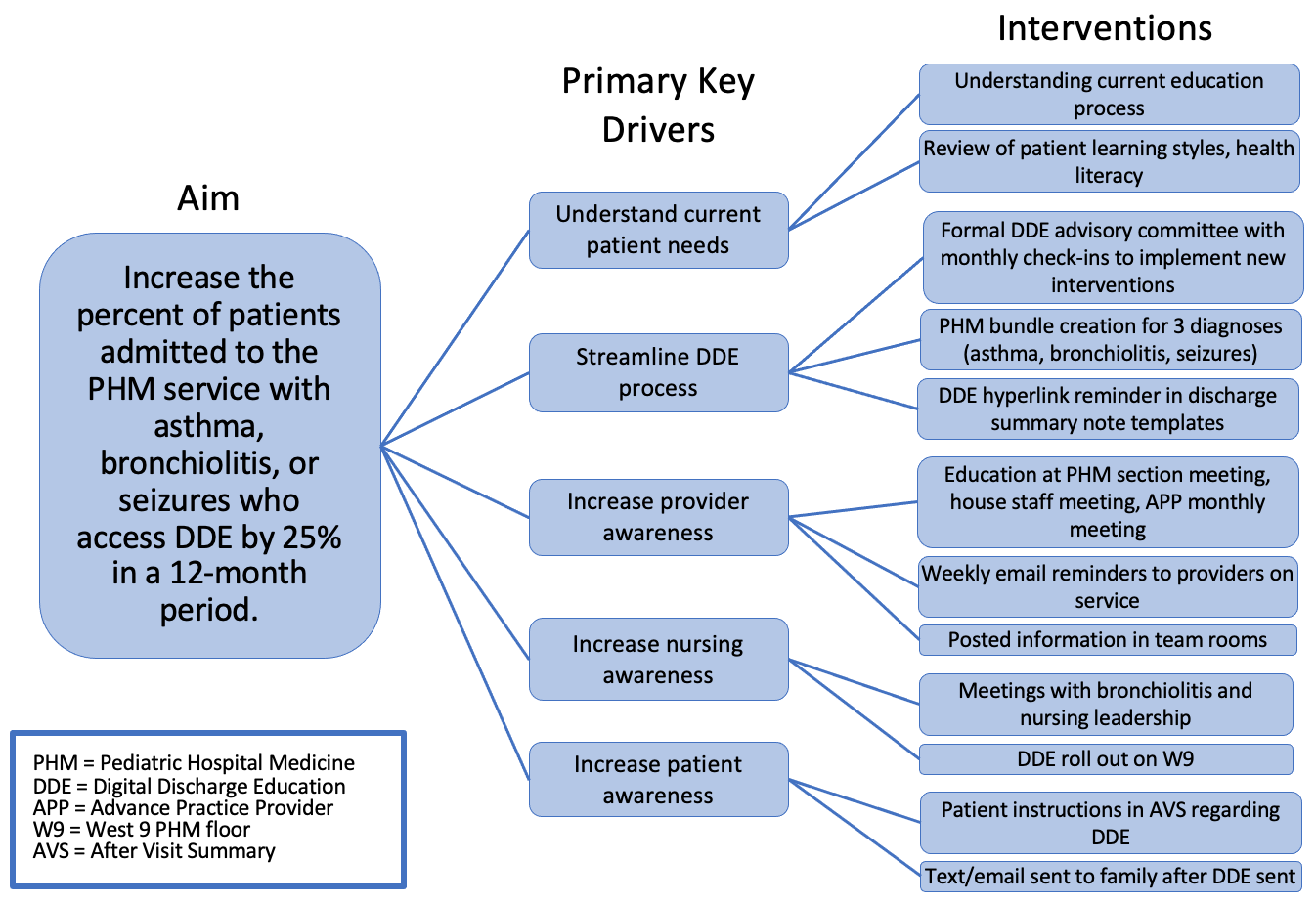
Methods: This quality improvement initiative took place at a 298-bed freestanding tertiary care children’s hospital. We created a key driver diagram to identify interventions to test to achieve our aim (Figure 1). The outcome measure is the percentage of PHM patients with the identified diagnoses that accessed DDE sent to the caregiver prior to discharge. The process measure includes the percentage of those patients who were sent DDE. The balancing measure is the percentage of patients who never access DDE that is sent. Plan-do-study-act cycles were conducted to test interventions. Statistical process control charts assessed the impact of interventions.
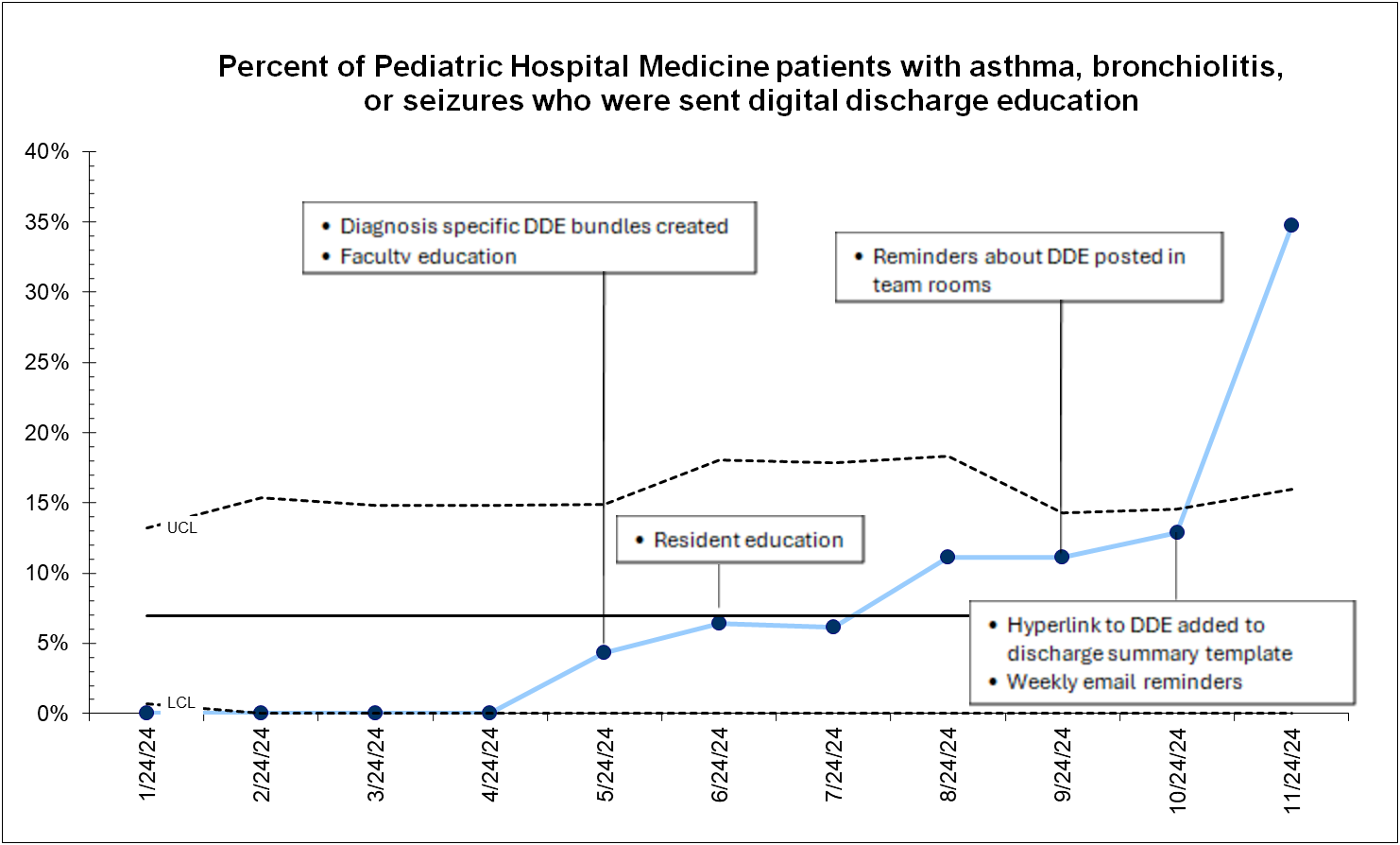
Results: 935 PHM patients with bronchiolitis, asthma, or seizures were discharged during the study period of January-November 2024. At baseline, no DDE was sent. 106 patients were sent DDE from May 2024 (the start of the intervention period) to November 2024. Only 87 patients (82% of the patient population) actually received DDE. Special cause variation in the process measure, or the percent of patients that were sent DDE, was seen after interventions of weekly education email reminders, and the addition of a hyperlink to DDE in the discharge summary template (Figure 2). Of those who were sent DDE, only 9.4% of patients read, watched, or listened to DDE.
Conclusions: While DDE is being reliably sent after numerous interventions, the majority of families do not access the material that is sent. Next steps include ensuring DDE that is sent is being received by families. We identified that some patients have non-smart phone numbers that are listed as the preferred method of communication. Further interventions to target include collaborating with staff to ensure mobile contact information for families to receive information. Additional next steps include exploring ways to automate sending DDE triggered through specific admission order sets for the identified diagnoses and engaging with nurses to send digital education themselves. Lastly, future studies should look to eliciting feedback from families who successfully receive DDE regarding their own barriers to accessing it.