Background: Intimate partner violence (IPV) is a serious and prevalent public health issue associated with increased healthcare utilization and worse healthcare outcomes. The majority of IPV outcomes research is conducted in emergency and outpatient populations. Our study aims to investigate how IPV exposure affects hospitalization rates and outcomes in adult patients.
Methods: We performed a matched case-control study of patients who were exposed to IPV and had at least one hospitalization at a tertiary care hospital between October 1, 2016 – October 1, 2019. We defined IPV exposure as patients who met at least one of the following three criteria: 1) Reported “yes” to a standardized, universal abuse screen performed by nurses at our hospital or affiliate clinic-based setting; 2) Received a referral to our hospital’s IPV advocacy program; or 3) Had an ICD-9 Code for IPV within the healthcare system. We defined controls as individuals who responded “no” to the standardized abuse screen and had at least one hospitalization during the same period.Each IPV-exposed patient (case) was matched to three unexposed patients (control), matched on sex, age range within five years, and location of abuse screening (inpatient, outpatient, or emergency). We performed matched regression analyses to evaluate the association between IPV exposure and hospitalization rate (number of hospitalizations per year), clustered by match group. We performed similar matched analyses on secondary outcomes including: mean length of stay (LOS), AMA discharge, mean pain scale score, receipt of diagnostic and surgical procedures, and one-time antipsychotic medication.
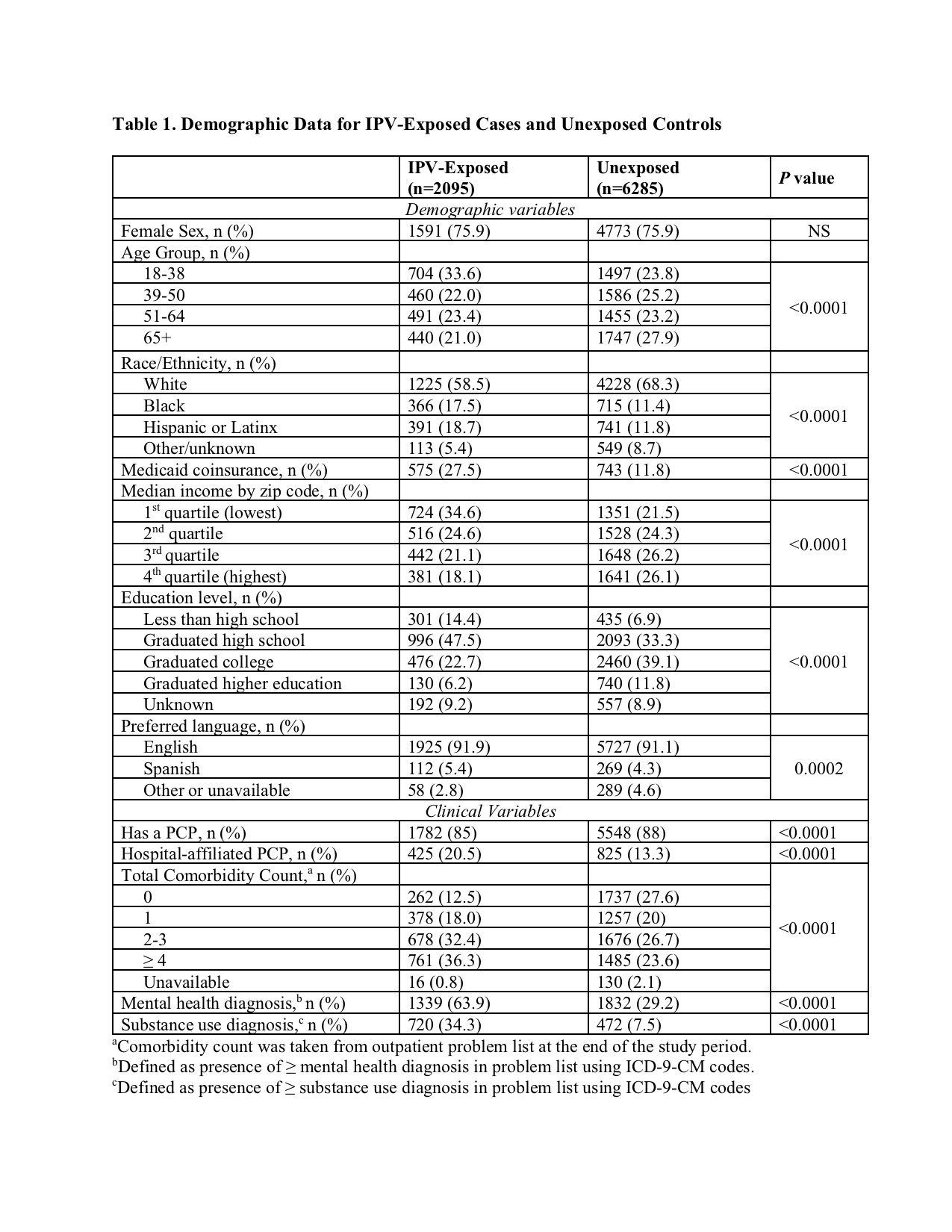
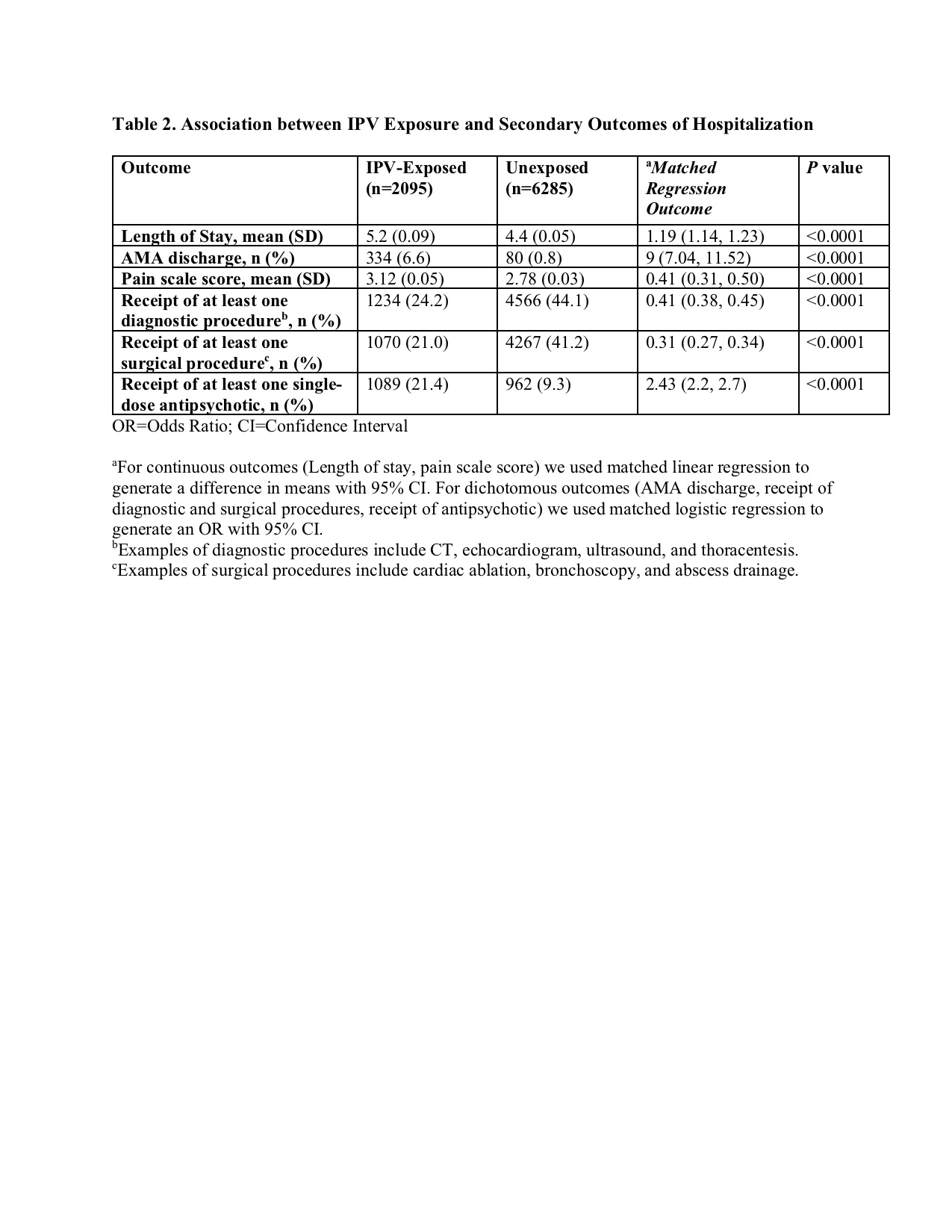
Results: Our cohort consisted of 2095 IPV-exposed cases and 6285 unexposed controls with at least one hospitalization in the study period, with demographic and clinical characteristics described in Table 1. There were 5093 total hospitalizations in IPV-exposed cases and 10347 in controls. In matched regression analyses, IPV-exposed patients had significantly higher hospitalization rates compared to unexposed patients (1.37 hospitalizations/year vs 0.88 hospitalizations/year, IRR 1.56 [1.16, 2.07], p=0.0325). Secondary outcomes (Table 2) similarly demonstrate significant differences between IPV-exposed and unexposed patients during hospitalizations.
Conclusions: We found that hospitalized adult patients with IPV exposure have higher hospitalization rates, longer LOS, greater mean pain scores, greater odds of AMA discharge, and greater use of single-dose antipsychotics compared to IPV-unexposed patients. Collectively these results suggest that IPV exposure is associated with both increased hospital utilization and greater hospital morbidity, complementing existing data on increased outpatient and emergency department utilization. Interestingly, we found that IPV-exposed patients are less likely to receive diagnostic and procedural care during hospitalization; this requires further research to elucidate the complex interplay of clinical and sociodemographic variables contributing to this observation, particularly in the context of higher reported pain scores. In summary, the findings of our study underscore the importance of targeted detection and intervention efforts for IPV in hospital settings in order to improve the care we provide to this vulnerable patient population.