Background: Patients with opioid use disorder (OUD) are frequently hospitalized, however up to 25% of these encounters end in patient directed discharge (PDD), leading to interruptions in care, increased mortality, and higher hospital readmission rates.1-4 Receipt of medications for opioid use disorder (MOUD) has been shown to decrease odds of PDD.5 However, to date, less is known about optimal timing and dosing of MOUD in hospitalized patients with OUD to decrease risk of PDD. We hypothesize that undertreated opioid withdrawal is associated with increased risk of early PDD and that higher dosing of MOUD within the first 72 hours of hospitalization will decrease this risk.
Methods: We performed a retrospective observational study of adult patients (>18 years old) hospitalized at Johns Hopkins Hospital from July 1, 2019 – June 30, 2022 with an OUD-related ICD-10 diagnosis in the electronic medical record (EMR). For patients with more than one hospitalization during the study period, only the most recent hospitalization was included. Patients who had a PDD > 72 hours after emergency department (ED) presentation were excluded. Patient demographics, hospital encounter details including time of ED presentation, Clinical Opiate Withdrawal Scale (COWS) score, and MOUD dosing and administration times were extracted by automated query from the EMR. The exposures of interest were COWS scores and MOUD administration doses and times. Only patients with oral and sublingual MOUD were included. The primary outcome was PDD.
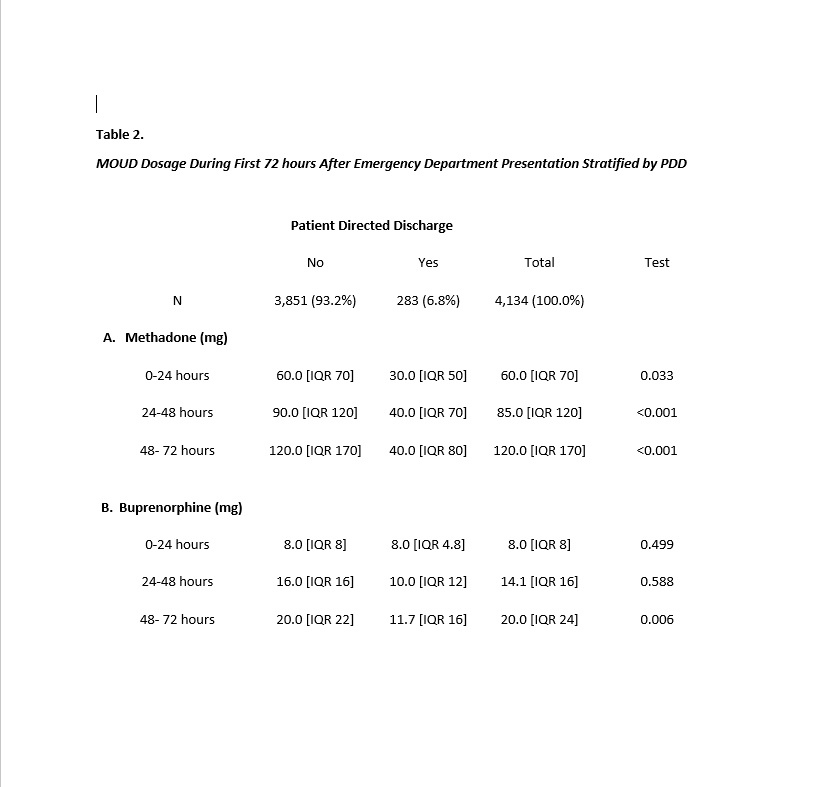
Results: 4,134 hospital encounters were included, among which 283 (6.8%) resulted in PDD within 72 hours of ED presentation. The median age was 37 (IQR 22). The cohort was majority male (57.5%), Black (58.2%) and had Medicaid insurance (59.3%). Over three-quarters of patients were admitted to a medicine service (76%). Similar percentages of patients received methadone (27.9%) and buprenorphine (23.6%) during hospitalization. COWS was implemented in over one-third of patients (35.8%). The median COWS prior to discharge was significantly higher in the PDD group (12 vs 2, p < 0.001). Methadone dose differed significantly between the PDD and non-PDD group for first 24 hours (30 mg vs. 60 mg, p = 0.033), first 48 hours (40 mg vs. 90 mg, p < 0.001), and first 72 hours (40 mg vs. 120 mg, p < 0.001). Buprenorphine doses differed significantly at 72 hours between the PDD and non-PDD groups (11.7 mg vs 20 mg, p = 0.006), but not at 24 or 48 hours (Table 2).
Conclusions: Our study findings support the hypothesis that undertreated opioid withdrawal (higher COWS) is associated with higher risk of PDD. There was a strong association with higher methadone doses in the first 72 hours with decreased risk of PDD, and for higher buprenorphine dose at 72 hours. More work is needed to understand safe and effective inpatient dosing strategies for MOUD, as well as the role of adjunctive medications and short-acting opioids.