Background: There has been conflicting data regarding the effect of comorbid asthma on severity of illness with COVID-19 disease. The prevalence of asthma reported in hospitalized patients as compared to the local population has varied widely across studies and areas of the world. Furthermore, the risk for testing positive for SARS-CoV-2 as well as the risk of increased clinical severity of COVID-19 has been shown to vary between allergic and non-allergic asthmatics in some cohorts. Our objective was to understand the impact of asthma as a predictor of disease outcomes in patients at two academic hospitals infected with SARS-CoV-2.
Methods: SARS-CoV-2 RT-PCR positive patients tested through our healthcare system were identified using an institutional informatics platform, and hospitalization status, asthma history, demographics, co-existing conditions, laboratory values and COVID-19 severity were determined. Inpatients were defined as those patients hospitalized within 14 days of a positive test for SARS-CoV-2. Patients were excluded from further analysis if they had no other documented clinical history or were younger than 28 days. COVID-19 disease severity was designated according to the 5 severity of illness categories from the NIH COVID-19 Treatment Guidelines.
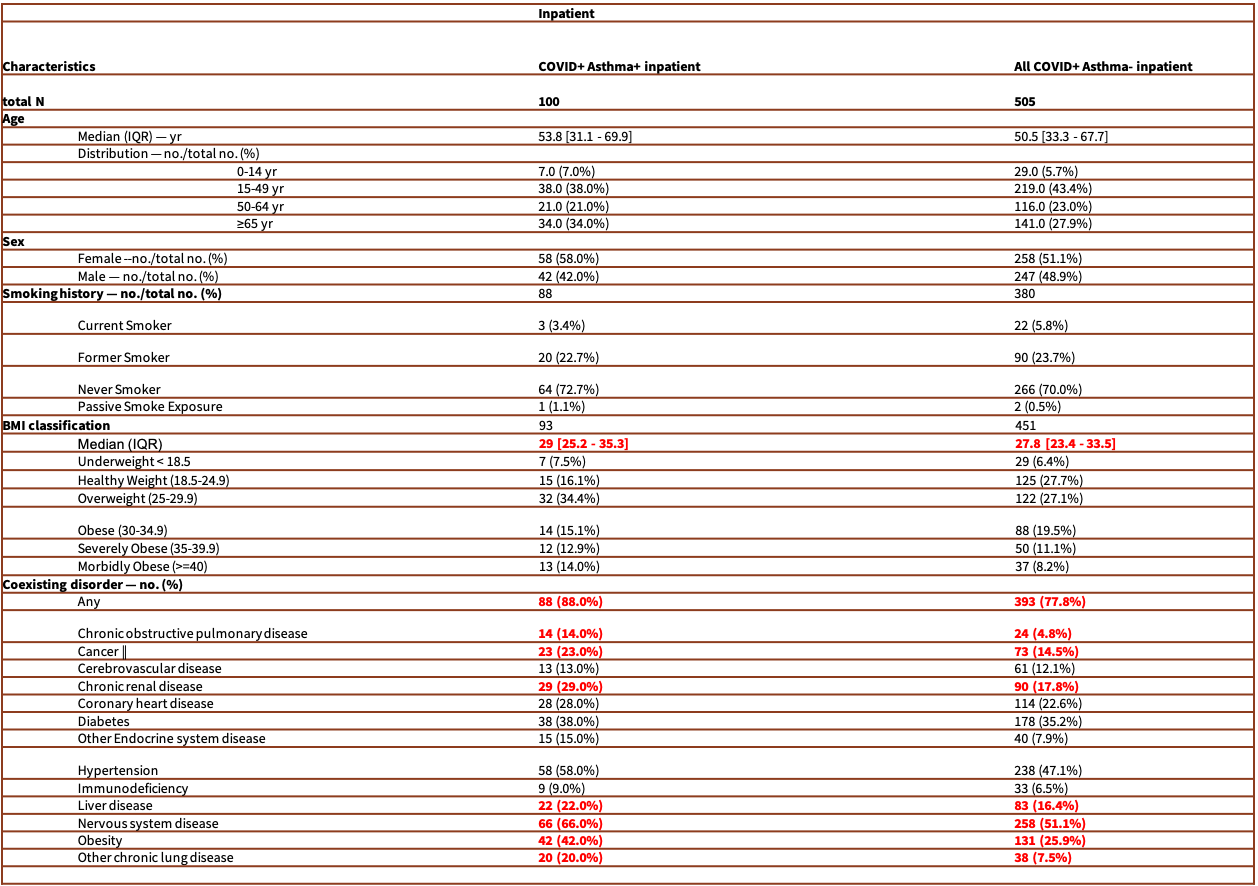
Results: From March 2 to September 30, 2020, 168,190 patients were tested for SARS-CoV-2 and 6,976 (4.1%) tested positive. 1,380 patients were excluded from further analysis. Of the remaining 5,596 patients, 605 required hospitalization. Of the 605 hospitalized patients, 100 had a pre-existing diagnosis of asthma. History of asthma was significantly associated with COVID-19-related hospitalization (p<0.001, adjusted odds ratio = 1.55, 95%CI = [1.21-1.97]) in multivariate analysis adjusted for age, sex, and ethnicity. Additionally, older age, male sex, and asthma were significantly associated with clinical severity of COVID-19 in hospitalized patients in multivariate analysis (p<0.05) with a trend for BMI >= 30 (p=0.06). For hospitalized patients with historical eosinophil counts (HEC) available for analysis, there was a trend toward higher HEC being protective for clinical severity (p = 0.075) stratified by age and asthma status.
Conclusions: In our cohort of 168,190 patients tested for SARS-CoV-2, 605 were hospitalized. A history of asthma was associated with need for hospitalization, and older age, male sex and asthma were significantly associated with increased clinical severity of COVID-19 disease in hospitalized patients. These data suggest asthma as a risk factor for COVID-19 disease severity in our study population.