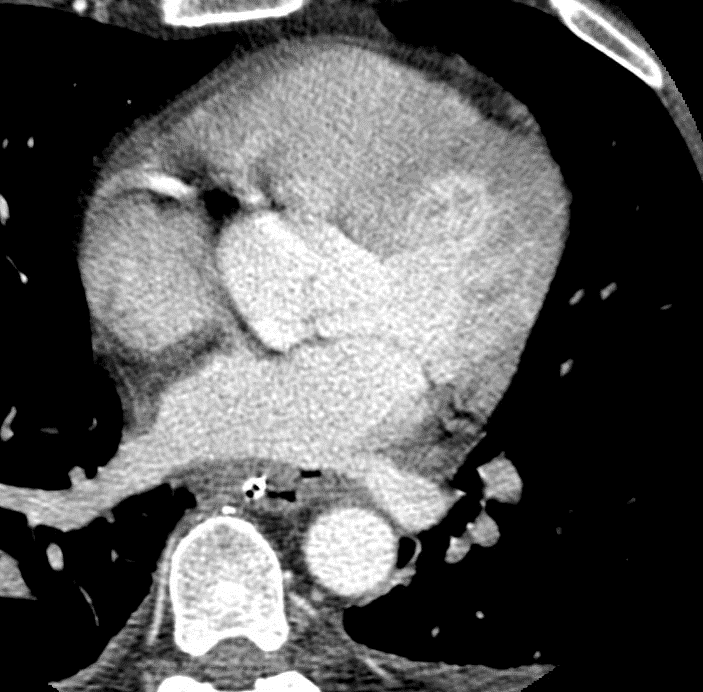
Case Presentation: 59 year old male with past medical history of paroxysmal atrial fibrillation status post radiofrequency ablation x2 who presents with fever, chills, left sided weakness, and hematemesis 2 weeks after a redo radiofrequency (RF) ablation. The patient initially presented to the outside hospital Emergency Department after developing fever, rigors, and nausea about 9 days after undergoing a cardiac ablation for his atrial fibrillation. Work up revealed streptococcal bacteremia and broad spectrum antibiotics were started. A CBC revealed a WBC of 10.8 and was otherwise normal. A complete metabolic panel was unremarkable. A transthoracic echocardiogram (TTE) suggested the presence of mitral valve vegetation and mild mitral valve regurgitation. He subsequently developed left sided weakness concerning for CVA. A CT Head and CT angiography of the head and neck were performed and revealed no abnormalities. MRI of the brain revealed acute tiny infarcts in an embolic distribution. His hospital course was further complicated by hematemesis. At this point he was transferred to the OSU WMC for further evaluation.Upon arrival we considered atrial esophageal fistula (AEF). A Cardiac CT was ordered revealed diffuse esophageal wall thickening with evidence of air outside the esophagus with a fistula track to the esophagus highly suggestive of esophageal perforation which is immediately adjacent to the left atrial wall near the left lower pulmonary vein ostium without contrast extravasation outside the left atrium or inside the esophagus. Cardiac surgery was consulted and repaired the AEF with pericardial patch and esophageal stent placement. All subsequent blood and operating room cultures were negative. Infectious Disease recommended a course of ertapenem and fluconazole. He was discharged on amiodarone, esomeprazole, atorvastatin, and apixaban. He was discharged with an NPO diet, tube feeding via PEG, and follow up with his cardiac surgeon.
Discussion: Esophageal perforation occurs in 0.1% to 0.25% of atrial ablation procedures and can develop into AEF. The mechanism of injury is thought to be related to esophageal heating resulting in thermal injury and ulceration, with fistulation occurring from the esophagus towards the atria. The signs and symptoms of AEF are not specific and may include fever, fatigue, malaise, chest discomfort, nausea, vomiting, hematemesis, melena, and dyspnea general occurring 1-6 weeks after AEF. Neurologic deficits and bacteremia are common and caused by the fistula allowing for bacteria and air to enter the blood stream from the esophagus to the bloodstream.When AEF is suspected a CT Chest with IV contrast should be ordered. If there is concern for AEF, TEE or upper GI endoscopy should be avoided as insufflation of the esophagus with air may result in large air embolus producing stroke or death.Management of AEF consists surgical repair and medical management of complications. Broad spectrum IV antibiotics should be started. NPO diet is started. Surgical approaches for AEF include biologic barriers/patches and esophageal stents.
Conclusions: AEF is a rare complication after the cardiac ablation. Signs and symptoms of AEF are not specific, and a high index of suspicion is recommended for all patients presenting with constitutional and neurological symptoms after an atrial fibrillation ablation. Early recognition, detection with imaging, and prompt surgical repair are required to prevent serious complications and death.