Background: Correctional insulin is frequently used in the hospital to optimize blood glucose levels before meals or even before bedtime. Dosages are not set and are instead scaled to the blood glucose level obtained just prior to administration. Insulin is considered a high-risk medication as dosing errors can potentially lead to serious adverse events such as hypoglycemia. In our hospital system, one of the hospitals already utilized a table-based order set in which the dosages were predetermined based on blood glucose ranges. Three of the hospitals used a formula-based order set in which nurses calculated the dosage based off the measured glucose level. Current guidelines recommend using a table-based dosing scheme in order to avoid medication errors. We thus created a new order set for our electronic medical record to change insulin dosing to table-based orders which was implemented system-wide.
Methods: Data was collected for all hospitalized patients > 18 years of age who received at least one dose of correctional insulin and were admitted to at least one of the four hospitals in the healthcare system between 08/26/2018 and 08/25/2019. The expected calculated dosage of insulin was based on the ordered formula or table and compared with the actual dosage administered to the patient. Dosing errors were defined as 1) over-treatment (if the dose given was higher than the ordered dose), 2) correct dose (if both doses matched), and 3) under-treatment (if the dose given was lower than the ordered dose). Errors which were recorded as a greater than 10 unit difference were eliminated from analysis as a manual review of these error types showed that it comprised only a small portion of total errors. Other errors that were excluded include orders which were incorrectly executed, encounters which occurred mid-transition, and errors in glucose measurement input at the time of administration.
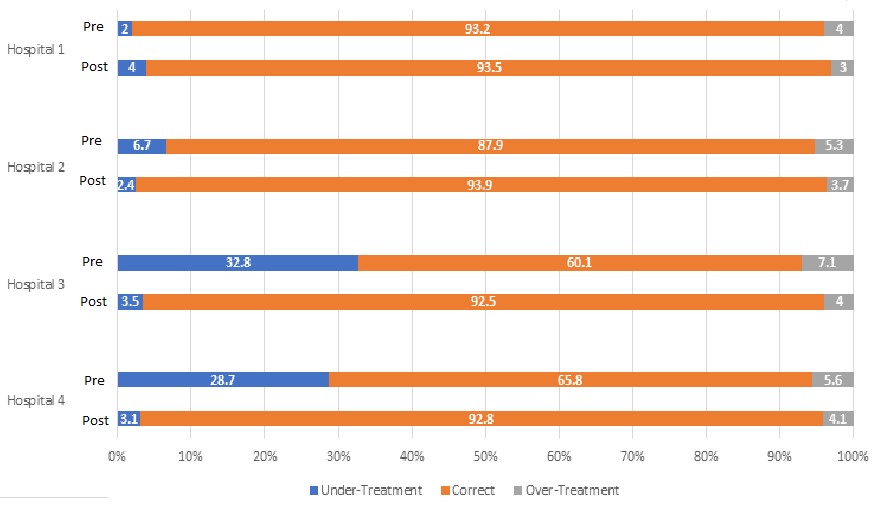
Results: In a system consisting of four hospitals, 88,556 corrective insulin doses were evaluated in the pre-intervention group compared with 98,109 doses in the post-intervention group for correct dosing. Hospital 1 already had table-based dosing in both the pre and post intervention groups and had unchanged measurements with 93.2% vs. 93.5% correct dosing in the pre and post intervention groups, respectively. With a transition from formula-based to table-based dosing, Hospital 2 showed an improvement from 87.9% to 93.9% (p <0.01), Hospital 3 improved from 60.1% to 92.5% (p < 0.01), and Hospital 4 improved from 65.8% to 92.8% (p < 0.01) (see table 1). The majority of errors which occurred were with under-treatment. Both under-treatment and over-treatment errors improved at all sites when switched from formula-based to table-based orders.
Conclusions: Changing from formula-based orders to table-based orders reduced the error rate of correctional insulin administration. It eliminated the need for performing calculations during busy shifts which could lead to increased errors. There was not a major impact on hypo or hyperglycemia from this change and more is needed to maintain glucose levels than just correctional insulin alone.