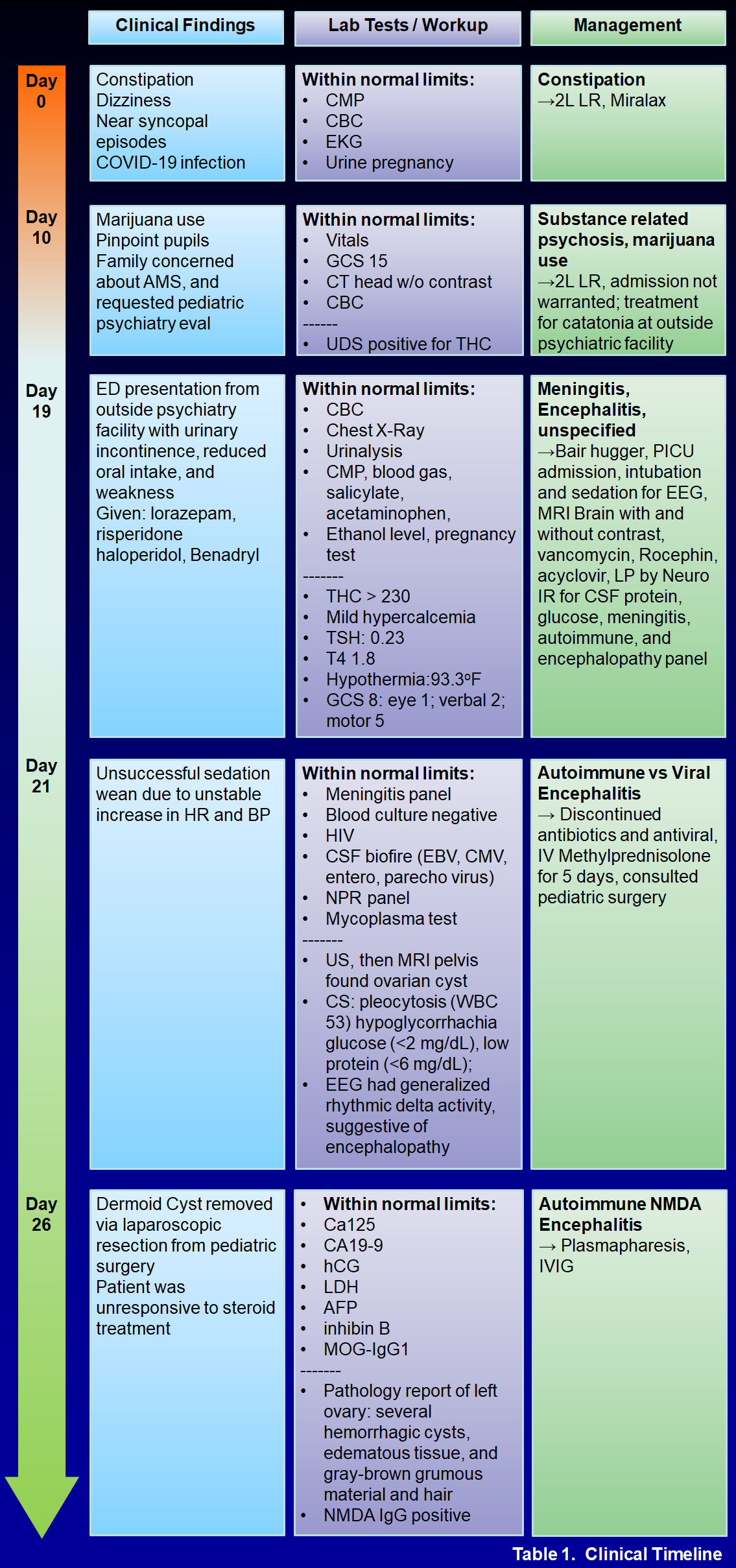
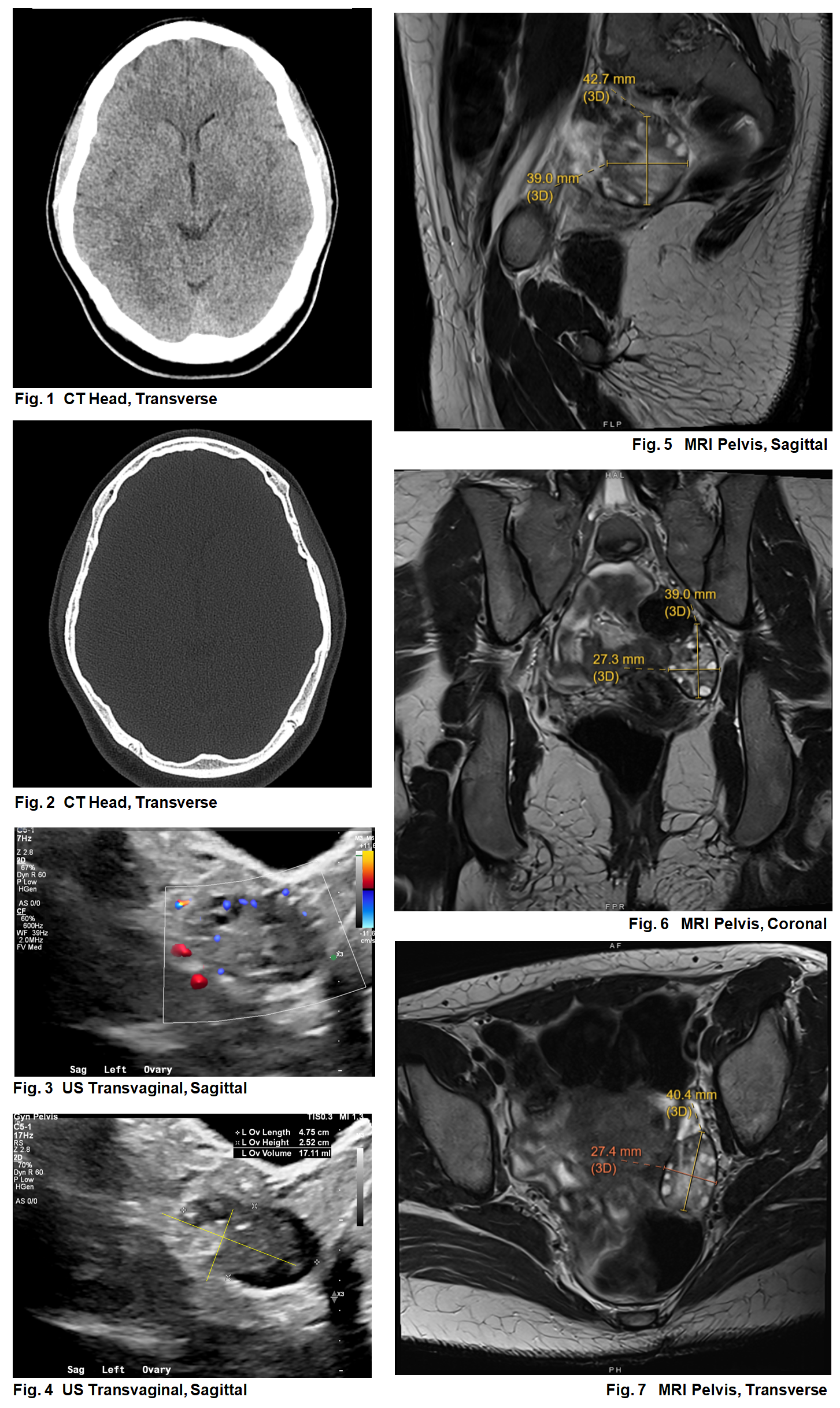
Case Presentation: A 17-year-old female presented to the ED with progressive encephalopathy. Three weeks prior, patient began experiencing pre-syncope, anorexia, increased sleep, and frequent urination. Her family described pressured, child-like speech. Patient endorsed smoking marijuana prior to symptom onset. History ascertainment was limited by her family’s inconsistent presence at bedside and her poor engagement during interviews. Patient had presented to and discharged from the ED 3 times for these concerns, with evaluation (CMP, CBC, toxicologic assays, urine pregnancy screen, non-contrasted CT head) notable only for +THC on urine drug screen. Psychiatry noted admission was unwarranted, and she was briefly admitted to an outside inpatient psychiatric facility for suspected drug-induced psychosis from family concerns. Over 3 days, she developed worsening confusion and urinary incontinence, prompting transfer to our ED. Upon arrival, patient was tachycardic (HR 101) and hypothermic (T 93.3 oF) with a Glasgow Coma Score (GCS) of 8 (eye 1, verbal 2, motor 5). Patient was sedated, intubated, externally rewarmed, and admitted to the PICU. The infectious workup was negative. EEG monitoring found rhythmic delta activity with lumbar puncture showing chronic lymphocytosis. IV methylprednisolone was started for suspicion of autoimmune encephalitis. Minimal response to steroids ultimately led to treatment with plasmapheresis, IVIg, rituximab, and further imaging. MRI pelvis revealed a left ovarian cyst. With the dermoid quality, CSF pleocytosis, and no infection, we confirmed our suspicion with a positive anti-NMDA receptor test. spurring a diagnostic/ therapeutic tumor resection revealing a 1x1x1cm gray-brown grumous material and hair-filled cyst. Patient gradually improved with multimodal regimens, allowing for extubation and subsequent care on the pediatric hospital medicine team. Persistent dysphagia, delirium, and agitation mandated ongoing multidisciplinary care and eventual discharge to inpatient rehabilitation at a facility with high psychiatric capabilities.
Discussion: Anti-NMDAR encephalitis (NMDARE) is the most common cause of autoimmune encephalitis. It presents as progressive psychosis, leading to seizures and potentially fatal autonomic dysfunction if untreated. While not exclusively neoplastic, it is associated with ovarian teratoma in about 1/3 of patients. Screening for ovarian germ cell tumors via pelvic ultrasound should occur in all female NMDARE patients, as early tumor resection is standard care. In this case, earlier diagnosis was challenging due to limited history and confounding drug use. Subacute onset of psychiatric symptoms with neurological signs should increase suspicion for encephalitis in pediatric patients.
Conclusions: Limited history and recent substance use complicated diagnosis of NMDARE from an ovarian teratoma. This case underscores the need to consider medical causes in altered mental status, especially in female patients with prior psychiatric records.