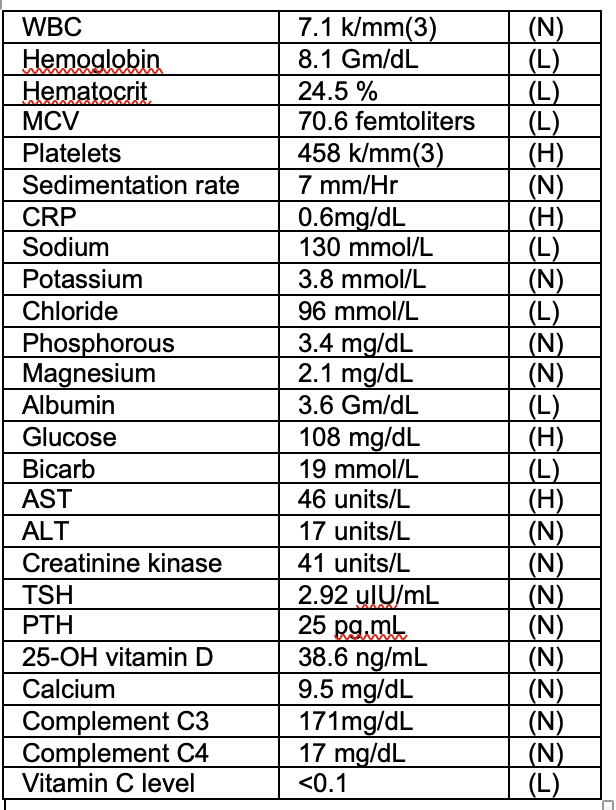
Case Presentation: Patient is a 4-year old male with history of developmental disorder who presented for primary concern of weight loss. Two months prior, patient developed left femoral metaphysis fracture following a collision with another child. He underwent casting. Following removal, he refused to bare weight on his lower extremities. Thereafter, patient developed bilateral leg pain with nocturnal wakening. Given concerns, patient presented to his medical home, with no cause for his symptoms identified. Approximately 3-weeks later, patient was re-evaluated and advised to present to the hospital due to 1.8kg weight loss.Patient endorsed leg pain and pain during handling. Family endorsed progressive irritability. They denied any symptoms consistent with malabsorption, malignancy or infection. History demonstrated severely restricted diet of yoghurt, home-made flat bread, raisins and water. Physical exam showed a thin, malnourished child. Oral exam showed dental decay, gingival bleeding. Patient had limited tolerance of passive limb movement. There was a perifollicular, raised rash on forearms. Patient was irritable, emotionally labile. Laboratory results showed microcytic anemia [Hb 8.1mg], iron deficiency [Fe level 31mcg/dL, Fe sats 11%]. UA showed 3+ Hb. ASOT, complement and US-renal were normal. X-ray of lower limbs showed healed fracture and diffuse bony demineralisation. Patients 25-OH vit D, PTH, calcium and phosphorous were normal. Given array of symptoms of mucosal bleeding, limb pain, irritability and peri-follicular rash, oral vitamin C was started. Following this, vitamin C level resulted as undetectable. Patient was diagnosed with scurvy and malnutrition. He gained weight with enteral feeding and had improvement in pain and behavior.
Discussion: Hospitalisations for pediatric scurvy have increased over the last two decades (1). Nutritional deficiencies can present in a variety of ways. Initial symptoms are often non-specific, including irritability and reduced appetite (2). Musculoskeletal symptoms include pain and limb swelling, which often manifests as refusal to weight bare in children (2). Mucocutaneous findings due to collagen deficits, include gingival bleeding and microscopic hematuria (3). Scurvy in resourced settings occurs commonly as a result of restricted diet in children with neurodevelopmental conditions (4,5). As this case shows, severe nutritional deficiency can worsen an underlying behavioural condition also (6). Treatment with vitamin C is considered safe and improvement in symptoms with treatment supports the diagnosis (7). Importantly, scurvy can occur with normal serum vitamin C levels and normal levels do not rule out the diagnosis. Additionally, scurvy can result in anemia via impaired absorption of iron and blood loss secondary to mucosal bleeding (2). Without appropriate vitamin C replacement, anemia as a result of scurvy can be fatal.
Conclusions: Hospitalisations related to severe nutritional deficiencies are prevalent amongst pediatric patients (8). Thorough dietary history in patients presenting with multi-system complaints remains crucial. While obtaining vitamin C level may be helpful, scurvy is a clinical diagnosis. Treatment with vitamin C is a low risk, high impact intervention which can improve symptoms and reduce hospital stay and investigations. Most importantly, the identification and treatment of scurvy can prevent progression to severe disease or death as a result of this uncommon, yet increasingly prevalent, disease.