Background: The Alliance for Academic Internal Medicine and the American College of Physicians have acknowledged the importance of POCUS in internal medicine for diagnosis and procedural guidance and support its integration into graduate medical education. There are no current standards for the content or structure of a POCUS curriculum. As a result, institutions looking to start POCUS educational curricula have independently done so within the limitations of their institution.
Purpose: We describe a novel POCUS education model consisting of complementary curricula implemented at our institution and report data from our first year.
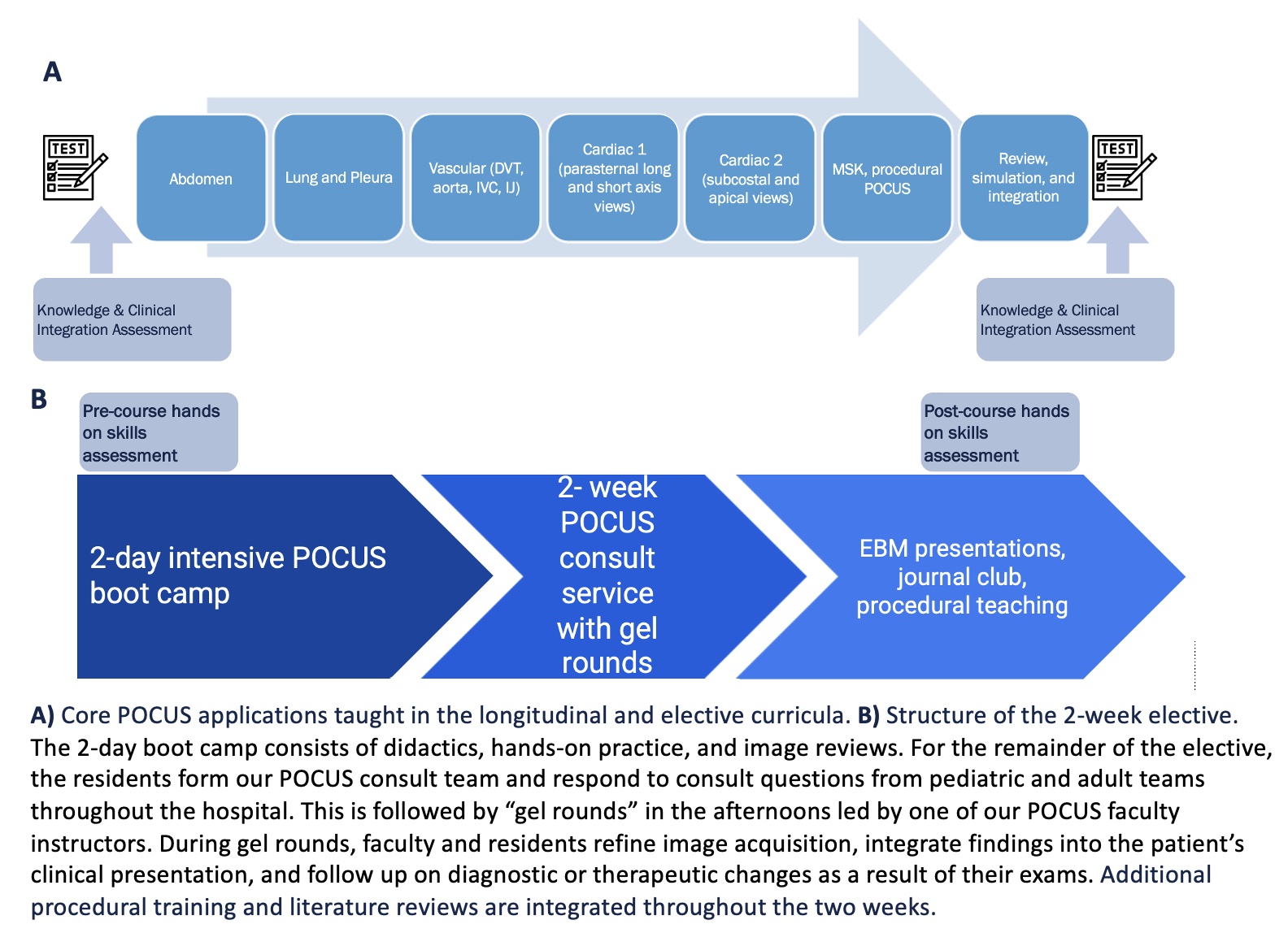
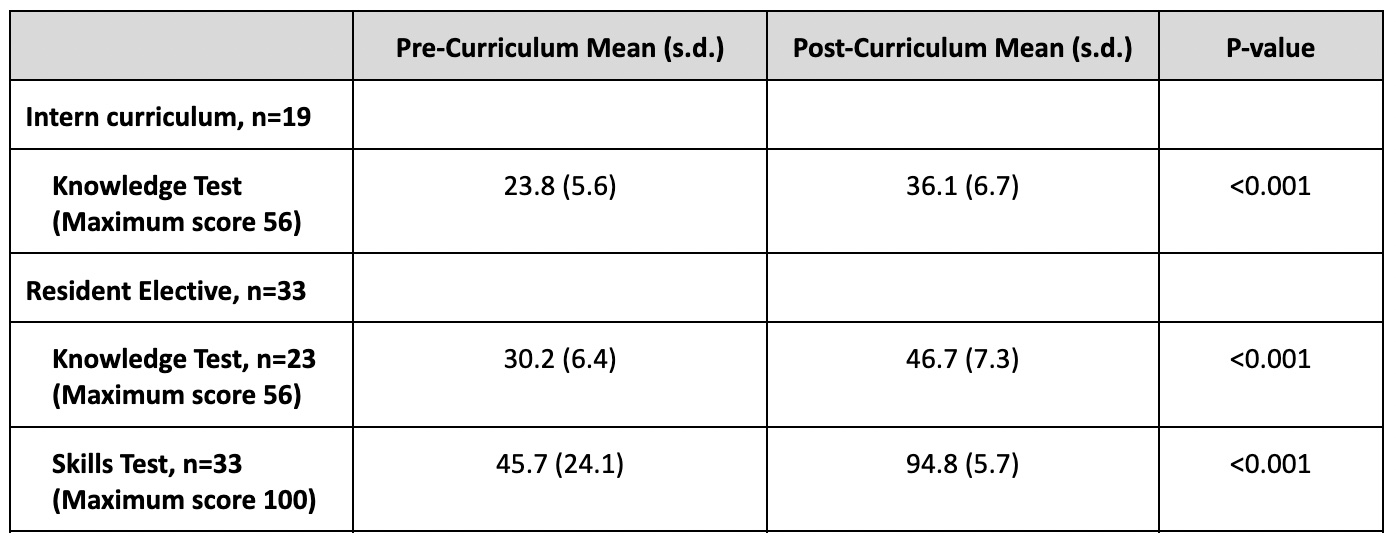
Description: For academic year 2021-2022, we developed a “Basal-Bolus POCUS Education Model,” which consists of a required longitudinal curriculum during the intern year (the “basal” component) followed by “boluses” of more intensive POCUS education throughout years 2-4. These boluses include a 2-week POCUS elective as well as reinforcement in the ICUs and wards, opportunities to teach the intern curriculum, and mandatory rotation on the procedure service to learn ultrasound-guided procedures. Our POCUS elective is interdepartmental, with participants from internal medicine, pediatrics, medicine-pediatrics, and family medicine residency programs. The basal, longitudinal component consists of a session every 6 weeks with a brief didactic of sonoanatomy followed by hands-on practice and abnormal image review. The educational sessions are shown in Figure 1A. Our elective structure is shown in Figure 1B.We developed a pre- and post- curriculum knowledge assessment, ranging from simple identification to interpretation and patient management. Trainees in the intern longitudinal curriculum and the upper-level elective are expected to take this exam before and after they complete the respective curricula. We adapted a hands-on skills assessment created by the Society of Hospital Medicine for the POCUS certificate of completion to evaluate trainee acquisition skills.We tested for differences in pre and post scores using paired t tests, with p-value< 0.05 considered significant. We taught 29 categorical medicine interns in our longitudinal curriculum. Of these, 19 completed the knowledge assessments and were included in data analysis. Knowledge assessment scores improved significantly post-curriculum (Table 1).We had 33 upper-level residents complete the 2-week POCUS elective. Of these, 32 elective participants completed the hands-on skills assessment and 23 residents completed the knowledge assessments. Both knowledge and skills assessment tests improved significantly post-curriculum (Table 1).
Conclusions: We developed a novel POCUS education model to address the growing demand for ultrasound teaching in GME in the face of limited faculty expertise, protected time, standardized curricular content, and trainee scheduling conflicts. This model provides baseline education during PGY1 year and opportunities for more intensive, focused training in subsequent years. Knowledge and skills testing shows significant gains after both “basal” and “bolus” curricula. Future study will show whether these gains are held and are additive over the course of resident training.