Background: Unrecognized in-hospital deterioration can lead to cardiac or respiratory arrests, and these events are often preventable. In pediatrics, in-hospital arrests are uncommon, making it difficult to identify risk factors or evaluate the success of interventions which aim to reduce unrecognized deterioration. In this study, we aimed to describe the demographic and clinical characteristics of hospitalized children who have an emergency transfer (ET) to an intensive care unit (ICU), a proximate measure of deterioration, and to determine the predictive validity of an ET on in-hospital mortality, ICU length of stay, and overall hospital length of stay.
Methods: We performed a retrospective-case control study of all ET cases at a free-standing tertiary care children’s hospital from 2013-2017. Emergency transfers, defined as any patient transferred from an acute care floor to an ICU where the patient received intubation, inotropes, or three or more fluid boluses in the first hour after arrival or before transfer, were identified from a hospital database and validated using manual chart review. To estimate the excess risk due to ET and not demographic- or disease-related factors, non-emergency transfers into the ICU were matched to controls on a 3:1 ratio based on age strata, hospital unit before transfer, and time of year. Patient demographics as well as number of medical conditions and specific diagnoses were abstracted as covariates. Outcome measures included in-hospital mortality, length of stay in the ICU, and post-event hospital length of stay. Chi-square testing was used to compare categorical outcomes, and Wilcoxon Rank-Sum testing was used for the non-normally distributed length of stay outcomes.
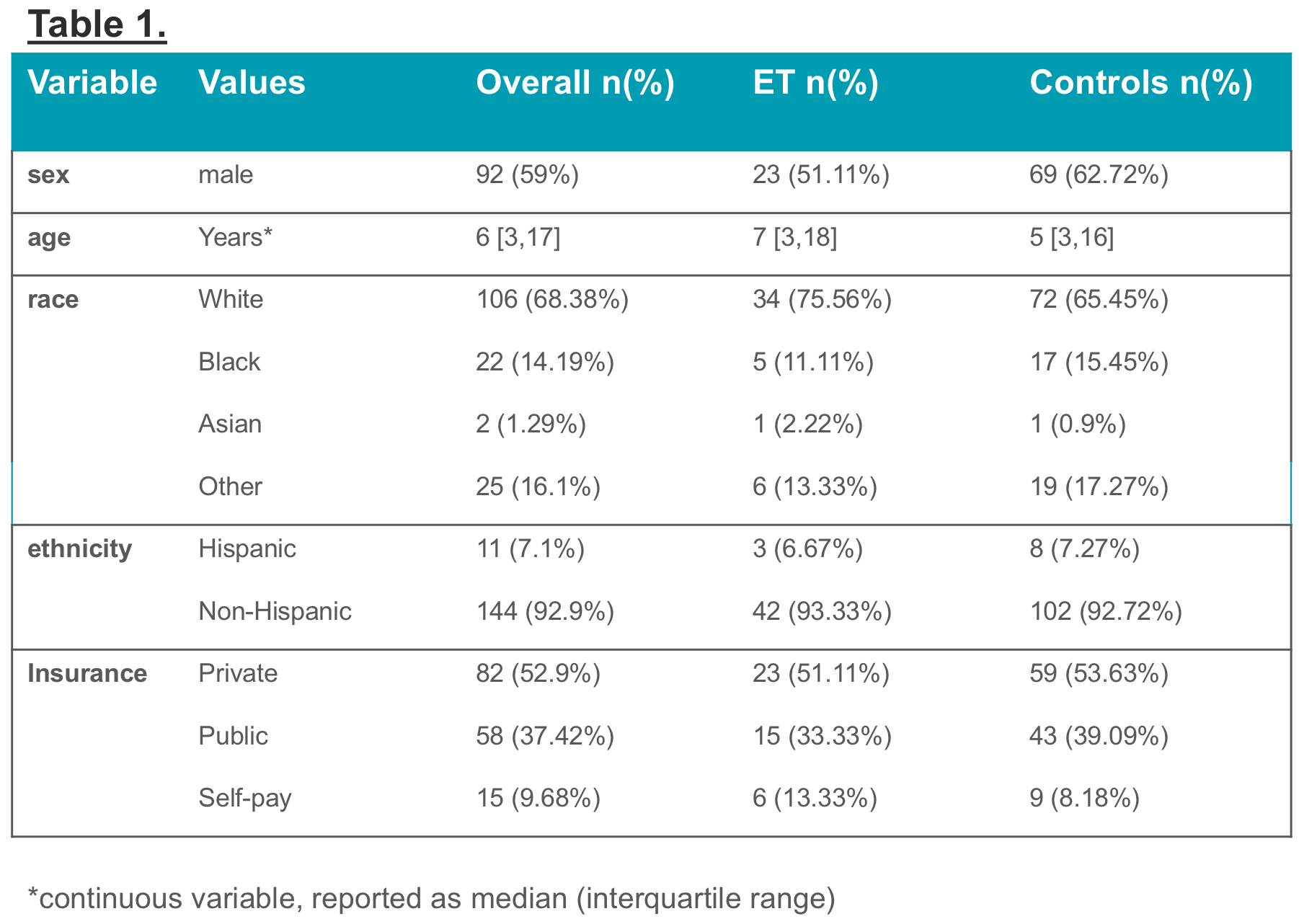
Results: A total of 45 ET cases and 110 controls were identified. There were no significant demographic differences amongst all cases and controls (Table 1). The in-hospital mortality rate was higher in ET cases compared to controls (22% vs. 9%, p=0.02). ET cases had a median ICU length of stay of 4.9 days, while controls had a median of 2.2. days in the ICU (p=0.001). The ET cases had a median hospital stay of 35 days post event, compared with a median 21 days of post-event hospital stay for controls (p=0.001).
Conclusions: Patients who experienced an emergency transfer had a higher likelihood of in-hospital mortality. These patients also spent a longer time in the ICU and in the hospital post-event as compared controls. The use of the emergency transfer metric in children’s hospitals may enable more rapid learning and systems improvement implementations.