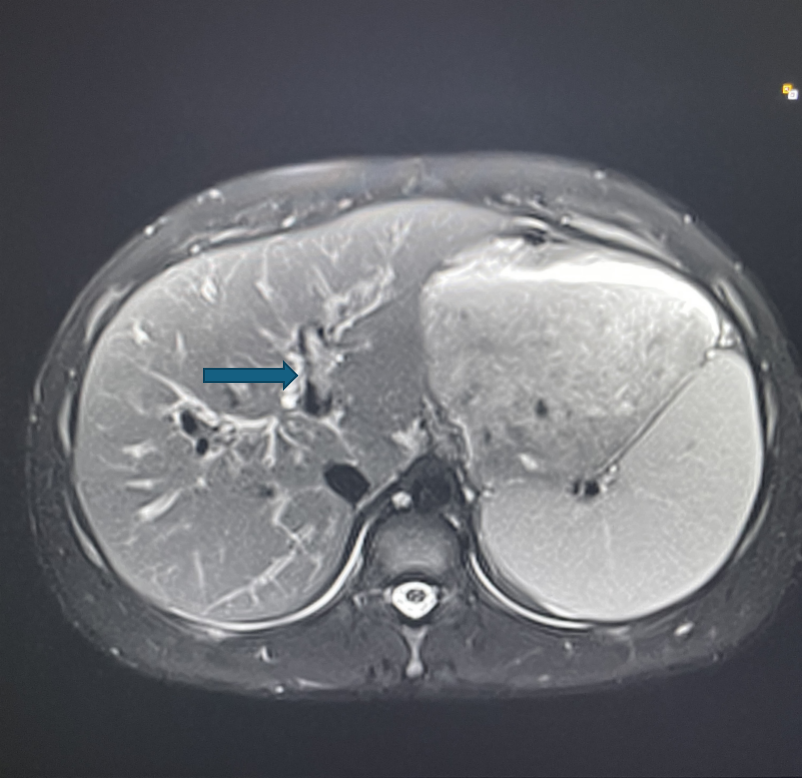
Case Presentation: We introduce a 17-year-old male with history of cholecystectomy two years prior, who presented to his pediatrician with transaminitis and hyperbilirubinemia. Workup revealed significant peripheral eosinophilia, along with elevated level of Immunoglobulin G (IgG). Autoimmune workup was significant for anti-smooth muscle antibodies and anti-neutrophil cytoplasmic antibodies (p-ANCA), but magnetic resonance cholangiopancreatography (MRCP) revealed a non-occlusive apparent thrombus in the left portal vein. Initially, the cause of transaminitis was thought to be the consequence of the non-occlusive thrombus leading to local ischemia versus inflammation (Figure 1). However, a liver biopsy demonstrated interface hepatitis consistent with AIH, confirming the diagnosis.
Discussion: This case represents a unique presentation of autoimmune hepatitis, peripheral eosinophilia, and portal vein thrombosis (PVT) in an adolescent. The coexistence of these etiologies is rarely described in literature. While AIH is recognized for causing immune-mediated hepatic inflammation, its link to thrombotic complications like PVT is not well established in children. In contrast, Hyper-eosinophilia can lead to thromboembolic complications as eosinophils can infiltrate tissues, release intracytoplasmic granules, such as eosinophilic cationic protein (ECP) and major basic protein (MBP), which can damage the endothelium and promote thrombosis. The presence of an apparent non-occlusive thrombus raised the possibility of localized ischemia, but the elevated autoimmune markers and histology suggested a more systemic immune-mediated process. This case highlights how a seemingly routine presentation of jaundice can reflect a multisystem disorder involving hepatic hematologic, and immunologic components. Hospital-based evaluation enabled timely diagnosis, prompt immunosuppressive and anticoagulant therapy, and ensured smooth transition to outpatient care.
Conclusions: This is the first case to our knowledge of simultaneous presentation of autoimmune hepatitis and a thrombotic event due to peripheral eosinophilia in the pediatric adolescent population. Given this novel presentation, further evaluation of similar cases should include autoimmune and hematologic testing, with targeted assessment for hypercoagulability when indicated. A comprehensive inpatient approach led to successful recovery, reinforcing the importance of collaborative care in pediatric autoimmune liver disease.