
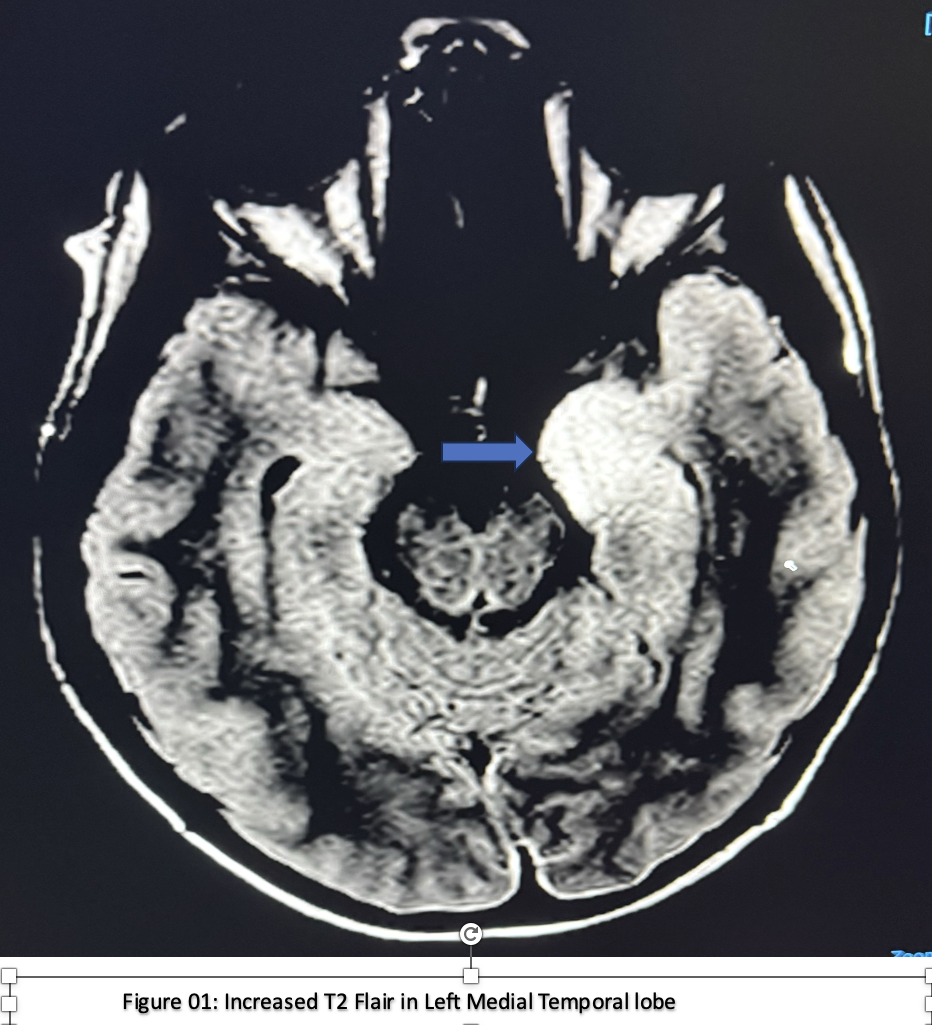
Case Presentation: An 11-year-old male presented to ED with complaint of bifrontal headaches initially brief and infrequent but progressing to 12 episodes per day. Headaches were associated with photophobia, left eye twitching and redness of both eyes. Initially, the team suspected cluster headaches, and he started on supportive treatment. The workup revealed leukocytosis with normal CT. However, his condition quickly worsened from frequent headaches to refractory seizures. An MRI showed an increased signal in the left medial temporal lobe and EEG revealed abnormal awake activity with spikes and waves in the left hemisphere and consistent with focal epilepsy without impairing the awareness. The patient was transferred to the PICU for management of status epilepticus. CSF and serum PCR were positive for HHV-6. His mental status declined despite being treated with antiepileptic medications and IVIG. Repeat MRI revealed cerebral venous sinus thrombosis. Extensive autoimmune and infectious workup was negative. Marked clinical improvement occurred only after initiation of corticosteroids.
Discussion: HHV-6 is typically associated with roseola in immunocompetent children, this case highlights a rare and severe neurologic complication: HHV-6 encephalitis complicated by status epilepticus and cerebral venous sinus thrombosis. The key diagnostic question was whether the disease process reflected active viral encephalitis or a post-viral autoimmune phenomenon. The lack of response to IVIG and improvement only after corticosteroids supported the latter. Additionally, the presence of hippocampal signal abnormality may represent mesial temporal sclerosis unmasked by HHV-6 induced inflammation. Infection-related inflammation is known to promote hypercoagulability, and while CVST is well-documented in HSV and VZV, HHV-6 has not previously been clearly linked. Still, the timing and clinical evolution support its role as a potential thrombotic trigger in this case. This case underscores the necessity of a multidisciplinary approach in the management of intricate pediatric presentations involving the convergence of neurologic, infectious, hematologic, and autoimmune processes. The marked improvement with corticosteroids suggests an immune-mediated mechanism, highlighting the need to further explore immunomodulatory strategies as potential therapeutic options in HHV-6–associated CNS disease.
Conclusions: This case depicts an uncommon occurrence of immunocompetent children developing HHV-6-associated encephalitis complicated by cerebral venous sinus thrombosis and refractory seizures. Antivirals like ganciclovir or foscarnet have been used to treat HHV-6 CNS infections in adult patients; however, there is currently no solid evidence to support similar treatment approach in children. The lack of evidence-based guidelines makes it difficult to choose the best course of treatment for pediatric patients.
.png)