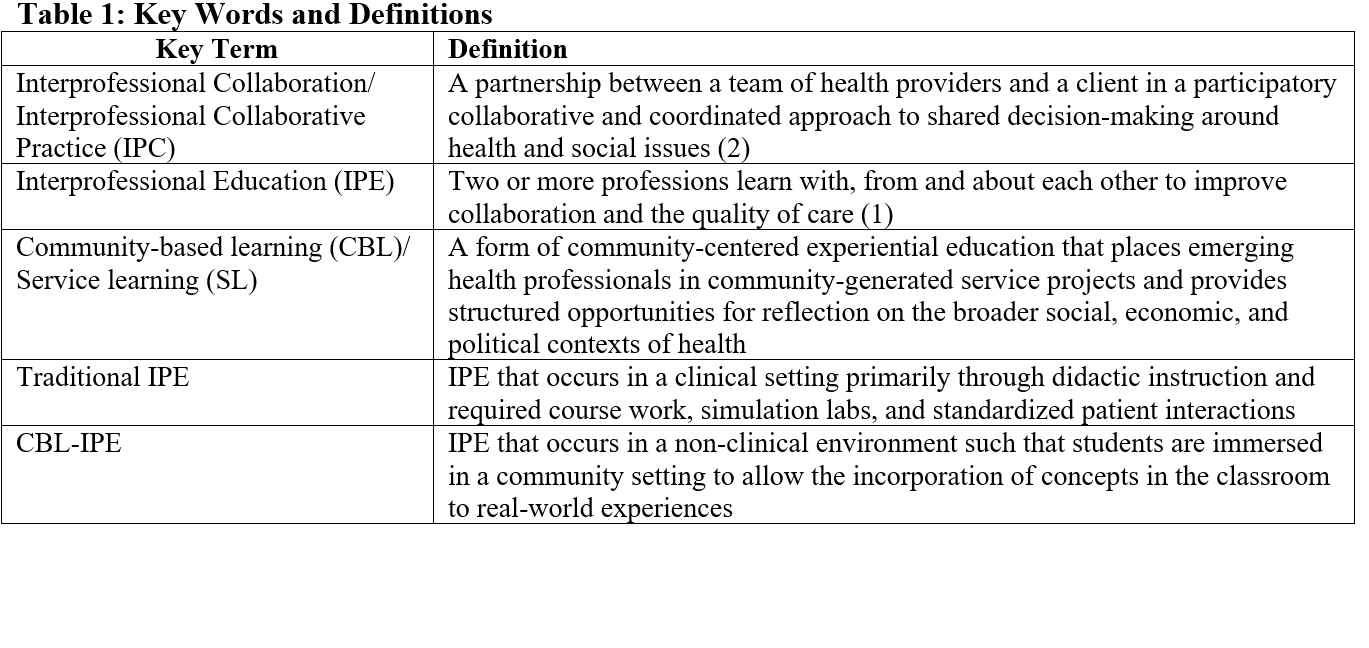
Background: Interprofessional Education (IPE) has been gaining momentum in academic institutions across the United States since the initiation of the core competencies of interprofessional collaborative practice (IPC). Research suggests that student learners who engage in IPE become interprofessional team members who respect others’ roles and work towards creating positive health outcomes. While the promise of IPE is great, implementation has often been challenging. Most institutions have integrated the IPE framework into their curriculum through didactic programs and interprofessional simulation experiences. Significant gaps in knowledge about IPE curricular interventions exist in non-clinical settings. This goal of this study is to review what is known about IPE and community-based learning (CBL), define and contrast IPE and CBL constructs, and describe advantages and barriers to an innovative approach that uses CBL as a framework for IPE.
Methods: In 2018, a literature review was conducted in PubMed on articles published between 2011 and 2018 utilizing the terms “interprofessional education (IPE)”, “Community-based learning (CBL)”, “medical education”, and “social determinants of health (SDOH)” to identify a body of published English articles relevant to the topic of interest.
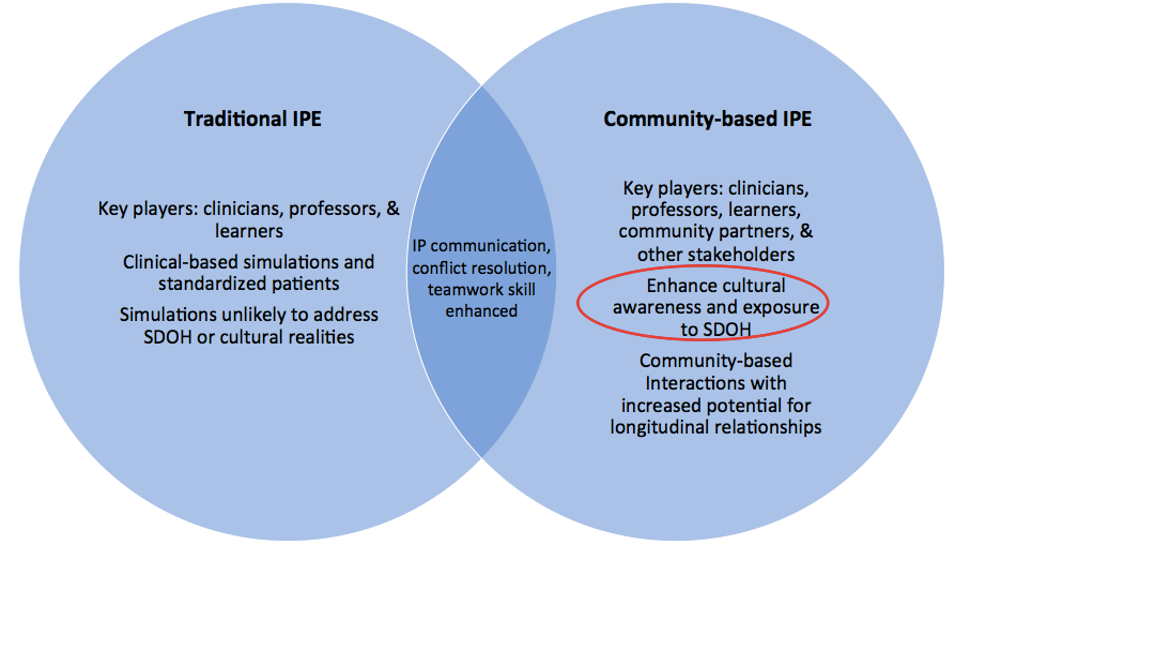
Results: This review reports on current IPE and CBL literature, barriers to IPE and CBL implementation, and an approach in incorporating CBL into an IPE framework. IPE is supported over the siloed methods of traditional medical education because it better reflects modern medical practice. The IPE literature proposes that the foundation for effective team-based professional health care is extensive interprofessional training at the academic level. Several barriers for implementing IPE including pedagogical barriers, logistical challenges, allocation of resources, deep-rooted hierarchical philosophies and culture, and resistance to change.CBL literature indicates that students who participate in this type of experiential education modality demonstrate statistically significant increases in five outcome areas: attitudes toward self, attitudes toward education and learning, civic engagement, social skills, and academic performance. Barriers to curating a meaningful CBL experience for students’ include restructuring curricula to accommodate CBL activities into schedules, coordinating with community partners, CBL instructors, and students to allow participation in CBL activities, and procuring long-term funding for CBL experiences.
Conclusions: While IPE alone has great promise to better train future healthcare professionals to function as a part of collaborative teams, incorporating CBL into the IPE framework has added benefits including expanding the interprofessional team, establishing longitudinal relationships, increasing exposure to SDOH, mitigating cynicism in caring for the underserved, and raising cultural awareness by engaging with communities foreign to most students. Through these programs, students would have the opportunity to have first-hand experience with SDOH, which are not traditionally explored with clinical IPE, and as a result, engage in finding solutions to real world problems. Exposing students to underserved communities early in their professional education could also increase their interest in working in these communities. Lastly, this novel approach to IPE will allow students to develop longitudinal relationships with patients and community partners.