Background: Hospitalists spend an estimated 30–40% of the workday documenting patient care encounters, yet this workload is not always captured through accurate billing and coding [1-2]. Billing guidelines revised in 2021 and 2023 simplified coding by focusing on medical decision making and expanding billing by time to include total encounter time instead of just face-to-face time [3]. However, many hospitalists were unaware of these changes. In general, medical training lacks education in coding and billing. Nationally, coding errors contribute to nearly $125 billion in lost revenue annually [4].
Purpose: In response to local financial pressure and observed documentation variability, we developed a billing and coding curriculum and an Epic dotphrase featuring a structured pull-down menu to streamline documentation, improve billing accuracy, and optimize reimbursement. A four-part curriculum was delivered in 15-minute segments over six months to all hospitalists across OHSU’s Division of Hospital Medicine. Educational content addressed the full billing spectrum for hospitalists. We delivered targeted instruction on accurate billing of admission and progress notes using medical decision making and total time spent, correct application of critical care and prolonged service codes, discharge documentation requirements, the difference between professional billing and hospital-based billing, and the use of precise diagnostic language to capture patient severity and complexity in diagnosis related groups (DRGs). We also introduced a standardized Epic dotphrase at the bottom of all inpatient notes that allowed providers to efficiently select key billing elements, including problem, data, and risk complexity at the point of care. A three-page educational summary of high yield points was distributed to all workstations in our team room for reference. Individualized feedback was provided to providers in the lowest quartile metrics on each billing topic throughout the intervention period. Participants completed pre- and post-education surveys. Billing specialists performed a comparative analysis of billing performance before and after curriculum implementation.
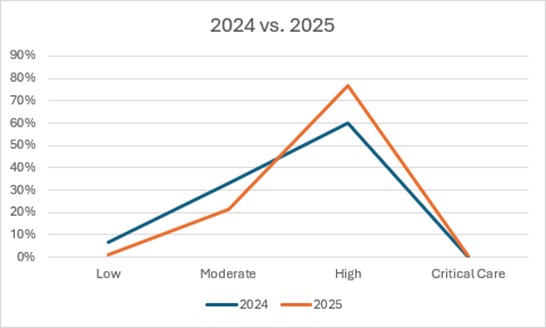
Description: Less than nine months after implementation, clinicians demonstrated meaningful improvements in billing performance and coding accuracy. The inclusion of time statements in discharge summaries increased from 60% to 83%, resulting in greater billing of the 99239 CPT code, and is on track for an estimated revenue gain of more than $39,000. The frequency of critical care billing rose by 130%, generating an additional $47,000. Level 3 billing (99223 and 99233 CPT codes) increased by 27%, while level 1 billing (99221 and 99231) decreased by 5%, which generated an additional $51,000. Overall wRVUs increased by 77% following implementation.
Conclusions: A targeted hospitalist-specific billing and coding curriculum led to substantial improvements in documentation practices and significant financial benefits within six months of implementation. This comprehensive approach ensured hospitalists were equipped to navigate the latest billing reforms, improved documentation quality related to billing requirements, and optimized reimbursements in the inpatient setting. Data continues to be collected with ongoing improvements observed. Education in core billing principles represents a scalable, high-value strategy for improving revenue integrity in not only hospital medicine, but in all inpatient departments.