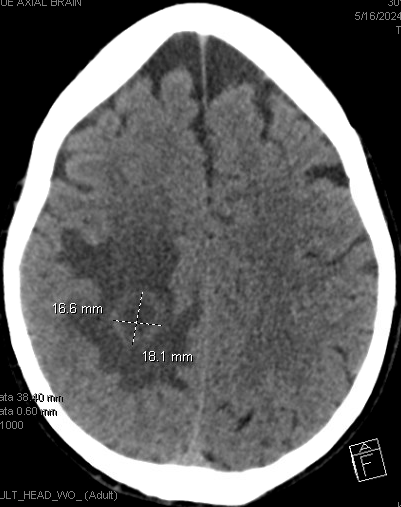
Case Presentation: A 64-year-old female with eosinophilic pneumonia, eosinophilic myocarditis, and hypothyroidism presented to the ED with four days of left upper extremity weakness. Symptoms began with a “sensation of heat,” progressing to left-sided weakness, impaired motor coordination, and fecal incontinence. She denied dizziness, visual changes, chest symptoms, falls, or head trauma.She previously used corticosteroids for eosinophilic pneumonia (last dose two years ago) and currently receives mepolizumab (IL-5 antagonist) every 28 days. Exam showed an anxious but well-appearing woman with intact cranial nerves, left triceps and grip strength of 4/5, no pronator drift, intact sensation, and normal coordination.CT head revealed a right parietal lobe mass. MRI showed a rim-enhancing white matter lesion. Biopsy found no malignancy, necrosis, or pus. On day 6, she underwent craniotomy with abscess evacuation, and cultures identified Cladophialophora bantiana (Dematiaceous mold).She was started on amphotericin and voriconazole, then voriconazole monotherapy. The patient was discharged with Infectious Disease follow-up for 6–12 months of treatment until radiographic resolution. Outpatient Allergy continued mepolizumab due to the risk of life-threatening hypereosinophilia with cardiac involvement.
Discussion: Black molds like C. bantiana are rare causes of intracerebral abscesses, with mortality rates up to 70% despite combined surgical and antifungal therapy1,2. This case highlights the complexity of managing a C. bantiana cerebral abscess in a patient with an eosinophilic disorder treated with immunosuppressive therapy. These abscesses present with varied neurological symptoms, making timely diagnosis and intervention critical1,3.Our patient’s use of mepolizumab, an IL-5 antagonist, raises questions about novel immunosuppressive therapy predisposing individuals to opportunistic infections. While mepolizumab controls eosinophilic conditions by lowering eosinophil counts and reducing steroid dependency, no direct link between mepolizumab and cerebral phaeohyphomycosis has been previously reported4,5.Unlike bacterial brain abscesses, fungal abscess management often demands radical surgical debridement, combined antifungals, and, when possible, immune recovery. Balancing aggressive antifungal therapy with careful immunosuppressive modulation is crucial to minimize relapse risk and prevent complications. Prolonged follow-up and repeated imaging are essential due to the risk of late relapses and challenges in achieving full radiographic resolution6.
Conclusions: Management of a C bantiana cerebral abscess in a patient on mepolizumab underscores the challenges of treating opportunistic infections in those receiving novel immunosuppressive agents. This case highlights the need for prompt surgical intervention, tailored antifungal therapy, and careful modulation of immunosuppressive medications, with ongoing monitoring to reduce relapse risk and improve outcomes. Further research is needed to understand the interplay between novel and infection risk, particularly in patients using biologics, and to establish thresholds for adjusting or discontinuing such agents during severe infections.