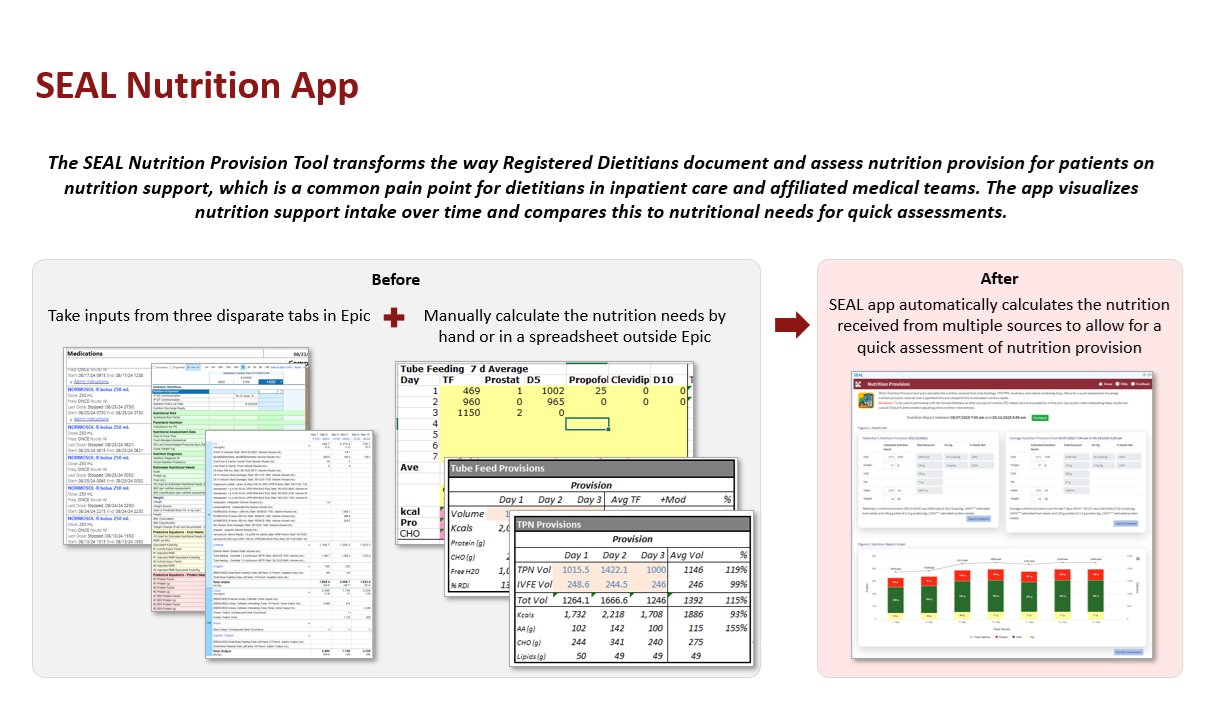
Background: The rigid architecture of electronic health records (EHRs) is inherently at odds with the dynamic environment of clinical practice, creating a widening gap between EHR workflows and frontline needs.(1) Although digital health solutions are available from external vendors, their implementation is often prolonged by legal and governance requirements, as well as architectural integration challenges, and they frequently struggle to progress beyond pilot phases due to a lack of deep understanding of local clinical pain points. Meanwhile, academic medical centers face similar difficulties developing and deploying internal tools, hindered by siloed governance, technical debt, and limited communication between developers and clinicians.(2) To bridge this implementation gap, we established SEAL, a cross-functional, agile product development team at our academic medical center designed to overcome traditional barriers and rapidly deploy clinician-centered solutions.(3) One of those is the Nutrition Provision tool, a clinician-designed app that has helped improve workflow and reduce burden for registered dietitians and affiliated medical teams.
Purpose: Our contributions include: 1) the deployment of an “embedded startup” operational model that integrates developers directly with clinical operations; 2) the utilization of SMART on FHIR architecture to create a native “app store” experience within the Epic EHR; and 3) the creation of a “Clinical Cabinet” to crowdsource problem identification directly from end-users.(4) We developed a portfolio of fifteen applications since 2021 through rapid prototyping and Plan-Do-Study-Act (PDSA) cycles.(5) For the Nutrition Provision tool, we conducted a deep-dive analysis, correlating app usage against documentation burden and time-on-task metrics using the Wilcoxon Signed Rank Test.(6) Impact was further assessed across the SEAL portfolio via usage logs for 1,981 clinicians and nearly 13,000 unique patients.
Description: The agile development model accelerated the “idea-to-deployment” timeline, processing over 50 intake concepts and launching thirteen stable applications with two in current development. In the case of the Nutrition Provision tool, the intervention yielded a statistically significant reduction in workflow friction: time-on-task completion decreased from a median range of 10-15 minutes to 5-10 minutes (p = 0.001, Z = -3.21, r = 0.76). Subjective assessments confirmed these gains, with self-reported documentation burden falling from a median of “somewhat burdensome” to “not at all burdensome” (p = 0.0005, Z = -3.51, r = 0.83). Across the broader portfolio, the lab successfully piloted other applications including artificial intelligence-driven (AI) billing and eConsult tools, scaling solutions that have improved care quality.
Conclusions: The novel application of a cross-functional, agile, in-house development team provides a scalable, objective method for overcoming the technical and administrative inertia common in large health systems. Our baseline data reveals that health systems can achieve significant reductions in clinicians’ cognitive load and administrative burden by lowering technical barriers and empowering clinicians to co-design solutions. The SEAL model demonstrates that rapid-cycle digital innovation is not dependent on massive institutional overhaul, but rather on establishing a dedicated, multidisciplinary infrastructure capable of responding to ever-evolving clinical needs.
.png)