Background: Medical emergencies present a major challenge to outpatient clinics. The University of Colorado Hospital (UCHA), a quaternary referral hospital with more than 1.4 million outpatient visits per year, previously relied on Emergency Medical Services (EMS) for patient evaluation and transport to the Emergency Department (ED), leading to prolonged response times, poor utilization of community resources, increased institutional costs, and a significant financial burdens for patients.
Purpose: In order to address these issues, we implemented a multidisciplinary Ambulatory Rapid Response Team (ARRT) led by Hospitalist APPs. This aligned with multiple institutional priorities: advancing patient-centered care, optimizing the emergency response through innovation, and promoting APP workforce development.
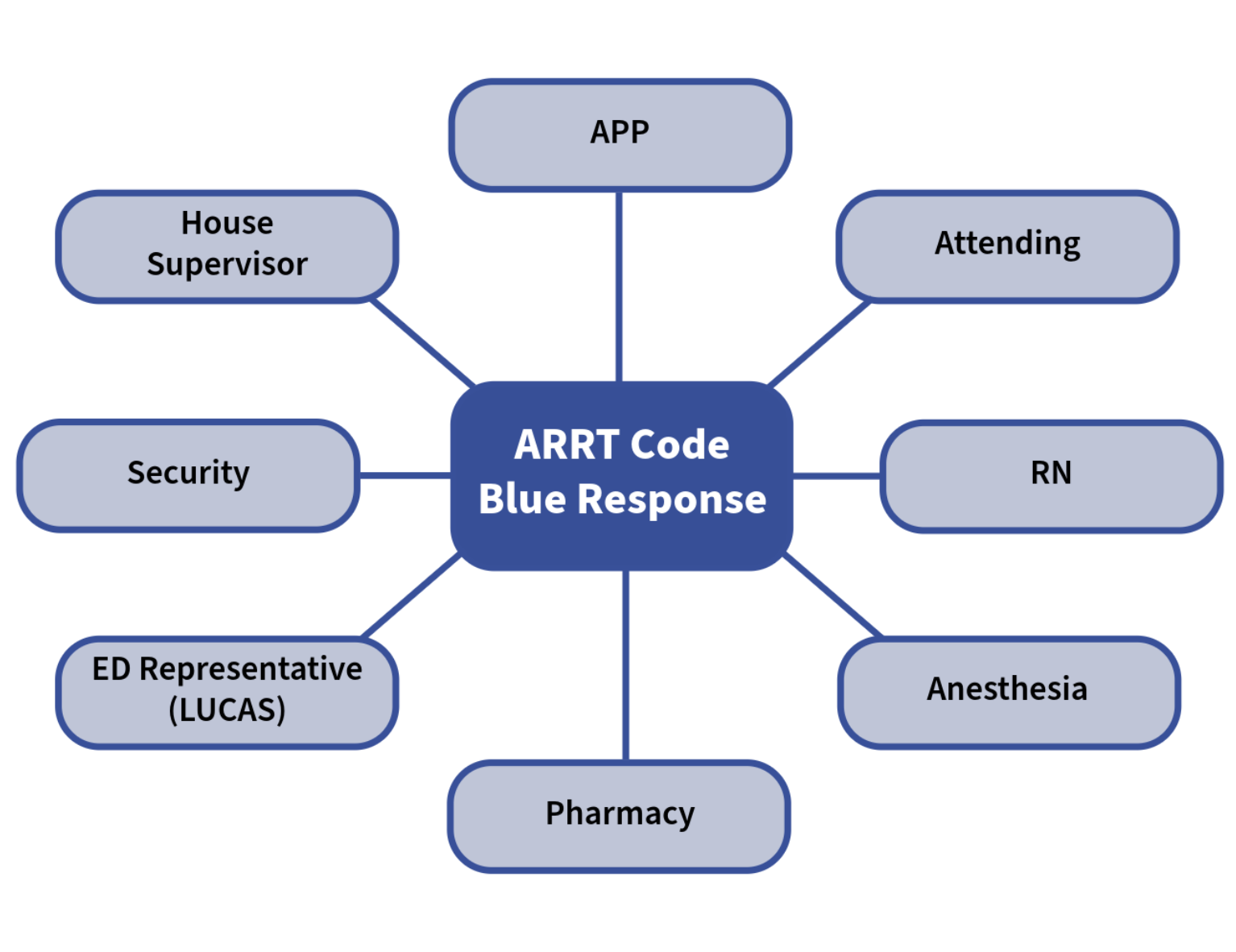
Description: The ARRT was deployed in 2020 and responds to an average of 61 rapid responses a month, with common chief complaints including Altered Mental Status, Falls, Hypotension, Syncope/Presyncope, and Respiratory Distress. The structure of the service includes Advanced Practice Providers (APPs) who split their time between a dedicated medicine consult service and responding to ambulatory rapid responses throughout the day. The team has access to equipment and medications for appropriate assessment and intervention in rapid response situations. Cardiac or respiratory arrests trigger a tiered response including Hospitalist Physician, Anesthesia, Respiratory Therapy, Pharmacy, and House Supervisor. To further support this initiative and address rising acuity in the ambulatory setting, a dedicated curriculum has been implemented for a core team of Ambulatory Rapid Response APPs, which has recently gone live in September 2025. During this curriculum, the core group performs bi-yearly mock code and high-fidelity simulation patient experiences to continue to expand upon the capabilities this team is able to offer. Structured case debriefings and collaborative reviews also take place. Finally, a comprehensive Ambulatory Rapid Response Handbook standardizes clinical approaches and serves as a ready reference for APPs and nursing staff. Prior to deployment, EMS response time was 15 minutes on average and total time to ED arrival was approximately 40 minutes. Most recent data demonstrates time between the ARRT page and provider arrival is 5.8 minutes +/- 3.1 minutes, with a time between page and end time averaging 24.4 +/- 13.7 minutes. The ARRT can triage patients and provide point-of-care assessment, initial airway management and oxygen therapy, intravenous access and medication administration, basic trauma evaluation and immobilization techniques, and ultimate risk stratification and clinical decision-making regarding disposition. Notably, the ARRT has the ability to discharge patients directly from the ambulatory setting –occurring in approximately 15% of all rapid responses.
Conclusions: A Hospitalist APP-led ARRT is a novel, efficient, and effective approach to solving the challenge of medical emergencies in hospital-adjacent outpatient care areas. The measurable improvements in response times, coupled with the ability to triage and resolve a subset of emergencies without transfer, highlight the program’s value both clinically and financially. The innovative curriculum initiatives ensure continual skill development and knowledge retention, fostering a team with both confidence and competence in high-stakes situations.
.png)