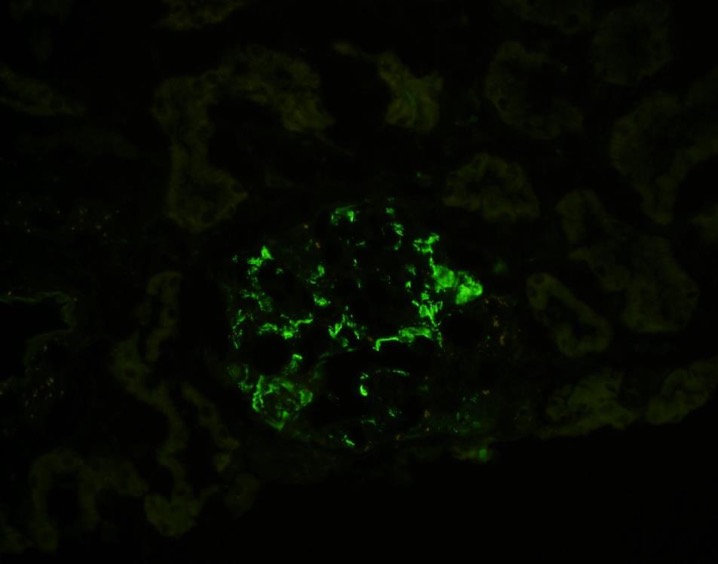
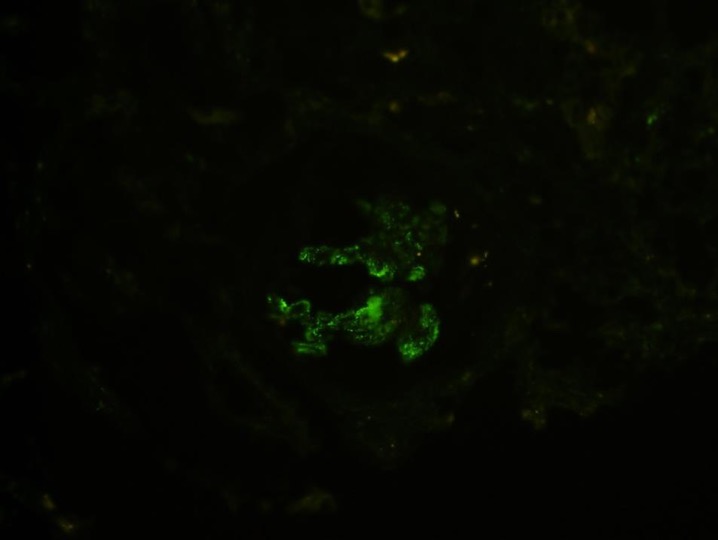
Case Presentation: A 29 year-old-woman was found to have proteinuria on routine labs that later progressed over the next few months to nephrotic syndrome with worsening lower extremity edema. Her work up revealed a positive (antinuclear antibody) ANA titer of 1:640. However, her anti-dsDNA and serum complement levels were normal, and she did not meet clinical criteria for Systemic lupus erythematosus (SLE) after extensive evaluation. A renal biopsy revealed pathologic features suggestive of C1q nephropathy, without classic features of lupus nephritis. Despite treatment with prednisone and cyclosporine over the next five months, her disease progressed leading to hospital admission for worsening volume overload. A repeat renal biopsy was performed for diagnostic confirmation. This biopsy showed evolution to focal segmental glomerulosclerosis (FSGS) with C1q nephropathy as well as diffuse foot process effacement of the podocytes in more than 90% of capillary loop surfaces. She continues on cyclosporine and is on a slow prednisone taper with reports of improved symptomatology, though she continues to have evidence of steroid-resistant nephrotic syndrome.
Discussion: C1q nephropathy is a rare immune-complex mediated glomerulopathy, thought to be a variant of FSGS, minimal change disease or mesangioproliferative glomerulonephritis. Current diagnostic criteria include 1) C1q electron dense deposits on immunofluorescence microscopy and 2) lack of clinical or laboratory evidence of SLE. There have been no reports of biopsy proven C1q nephropathy with a positive ANA titer. We treated our patient with prednisone and cyclosporine. Lack of clinical improvement led to a repeat renal biopsy, which demonstrated C1q deposition with progression to FSGS. This patient will be closely monitored for potential development of SLE in the future.
Conclusions: C1q Nephropathy is a histopathologic diagnosis characterized by dominant immunofluorescent staining for C1q electron dense deposits on renal biopsy in addition to the lack of clinical and serologic markers of SLE. In our case, a 29-year-old woman presenting with nephrotic syndrome was found to have C1q nephropathy on renal biopsy with a positive ANA titer, which led to a diagnostic conundrum. This led to a sebsequent biopsy again confirming C1q nephropathy. This may shed light on a new variant of C1q nephropathy or prove to be a risk factor in the development of SLE in due course.