Background: Improving efficiency and throughput in cancer patients with high acuity is challenging and requires a multi-disciplinary effort to coordinate care delivery. In The James Cancer Hospital, two separate Internal Medicine Divisions (Medical Oncology and Hospital Medicine) have historically provided inpatient oncology hospitalist care to an average daily census of 98 patients throughout The James, often across 7 different floors. To improve the quality and efficiency of care delivered to solid tumor patients, the Divisions of Hospital Medicine and Medical Oncology aligned to reorganize the inpatient oncology hospitalist program and to geographically localize patients.
Methods: A diverse team of stakeholders was formed and an iterative DMAIC methodology employed to identify solutions to optimize service line alignment and patient placement. The average daily census over a 6-month period was reviewed to delineate the footprint of current solid tumor patients and to minimize displacement of other services with localization efforts. Triage and bed placement rules were reviewed and adjusted. Metrics targeted included patient localization accuracy over time, length of stay, time from Emergency Department (ED) admission request to inpatient bed assignment, time from ED admission request to James bed arrival (as a surrogate for boarding hours).
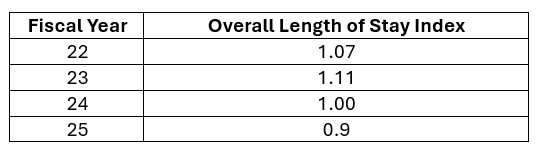
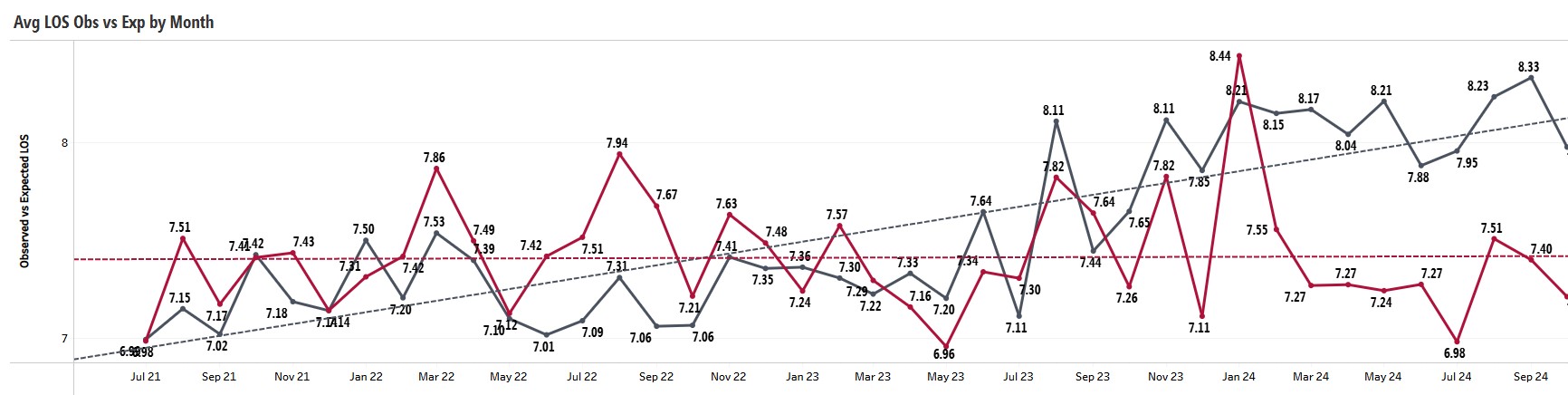
Results: On November 14th, 2023, the 7 services co-managed by the Divisions of Medical Oncology and Hospital Medicine were dissolved. While maintaining the same patient capacity, a new, cohesive solid tumor hospitalist program was launched, ‘Cancer Medicine’ (CM). Standardized triage and bed placement rules were adopted. Geographic patient localization was achieved across 7 inpatient units and maintained over time with >95% unit placement accuracy (December 2023-October 2024). The majority of a service’s patients continue to be isolated to a single unit and floor. Significant improvements in efficiency and patient throughput have been achieved. Since the project’s go live, the length of stay index (LOSi) for oncology hospitalist patients (all dispositions and length of stay groups) is at its lowest of the past several fiscal years (Table 1); the observed LOS has also declined since the intervention start (Figure 1). Time from ED admission request to bed assignment significantly (p=0.0008) improved, as did time from ED admission request to James inpatient bed arrival (p=0.0003), a surrogate for ED boarding hours.
Conclusions: The Cancer Medicine initiative resulted in the achievement of geographic localization of solid tumor patients, a new programmatic identity, and significant improvements in efficiency and throughput metrics. This optimization represents an opportunity gain for the larger health system, more cohesive care provision, and better access for solid tumor patients requiring inpatient care.