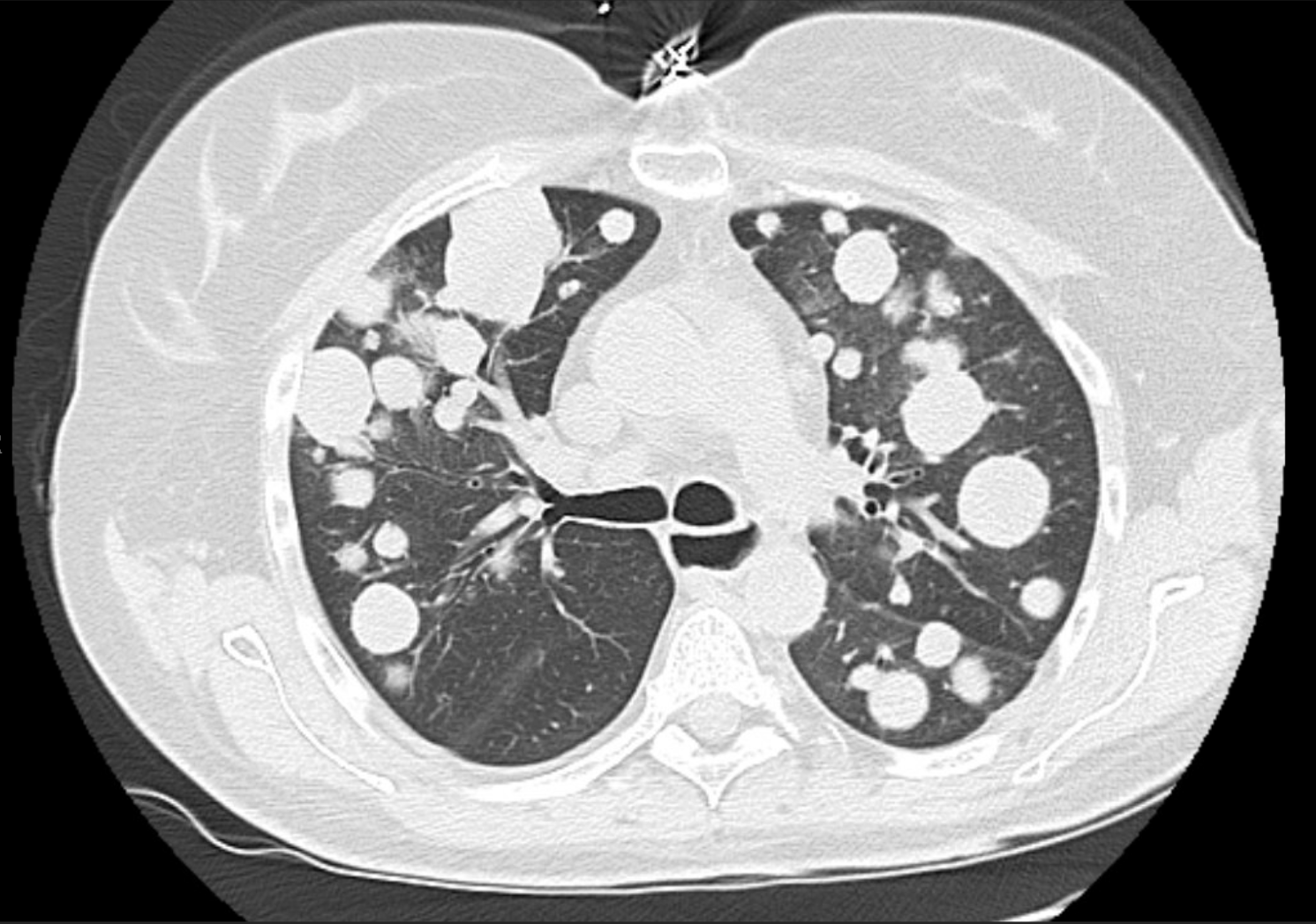
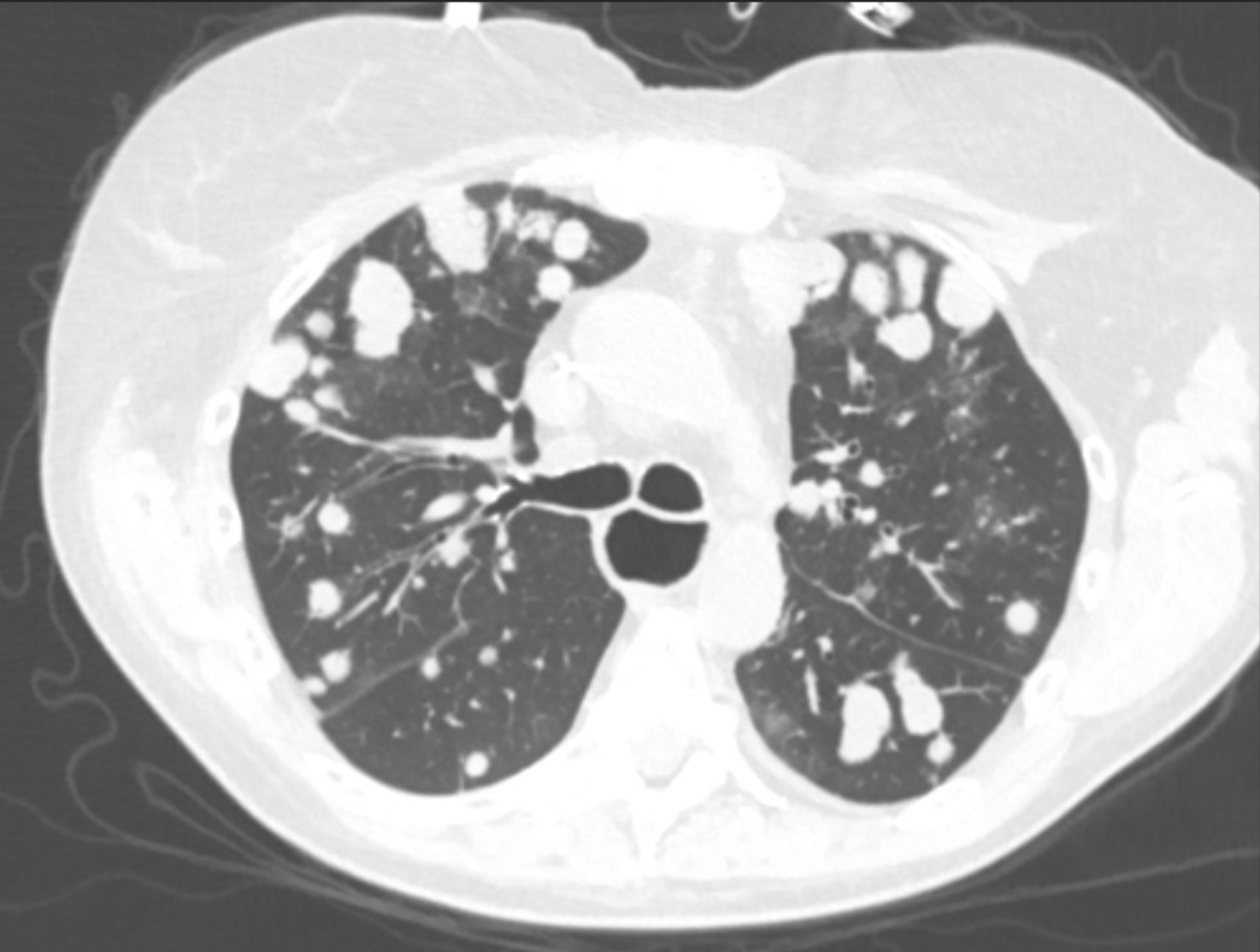
Case Presentation: We present the case of a 60-year-old immunosuppressed female with a history of simultaneous pancreas-kidney transplant who was initially diagnosed with CD30-positive pcALCL after a biopsy of a chronic non-healing wound on the right lower leg. Initially, she was treated with localized radiation therapy, achieving partial cutaneous response. However, after two months she developed progressive dyspnea and non-productive cough. This was attributed to allergies; however, the dyspnea progressed, prompting a presentation to a community hospital. The patient was hypoxic to 90% on room air, and CT chest revealed innumerable bilateral pulmonary nodules with a classic “cannonball” appearance. She was transferred to a tertiary care hospital. Bronchoscopy with endobronchial ultrasound-guided biopsy confirmed pulmonary metastases of CD30-positive, ALK-negative anaplastic large cell lymphoma—supporting transformation from pcALCL to systemic disease. She started systemic chemotherapy with Brentuximab Vedotin plus CHEP (cyclophosphamide, doxorubicin, etoposide, prednisone). Her hospital course was complicated by tumor lysis syndrome, toxic/metabolic encephalopathy, and multiple infectious complications including bacteremia and C. difficile colitis. Despite these setbacks, she remained clinically stable, had improved performance status, and resumed therapy after a brief delay.
Discussion: Primary cutaneous anaplastic large cell lymphoma (pcALCL) is a rare, CD30-positive cutaneous T-cell lymphoma that typically follows an indolent course and remains confined to the skin. Visceral dissemination is exceedingly rare, reported in fewer than 2% of cases. Transformation to systemic ALCL (sALCL), particularly with pulmonary metastases, is poorly understood and associated with poor outcomes. Although primary cutaneous anaplastic large cell lymphoma (pcALCL) is typically considered an indolent lymphoma confined to the skin, rare cases of systemic progression—including visceral metastasis—have been documented. Only a single case was identified in which biopsy-proven pcALCL metastasized to the lungs. The patient, an 81-year-old woman, expired after only two cycles of chemotherapy, highlighting the poor prognosis once systemic dissemination occurs.
Conclusions: This case highlights a rare and clinically significant transformation of pcALCL into systemic ALCL with pulmonary metastases and is the first of its kind to document this in a transplant recipient. The patient’s ALK-negative status, immunosuppressed background, and rapid visceral progression underscore the need for heightened clinical vigilance in managing pcALCL, specifically in transplanted patients. While pcALCL typically follows a favorable course, this report demonstrates that systemic dissemination—though uncommon—requires urgent recognition and transition to aggressive systemic therapy. Early detection and further research into predictors of transformation are essential for improving outcomes in this population.