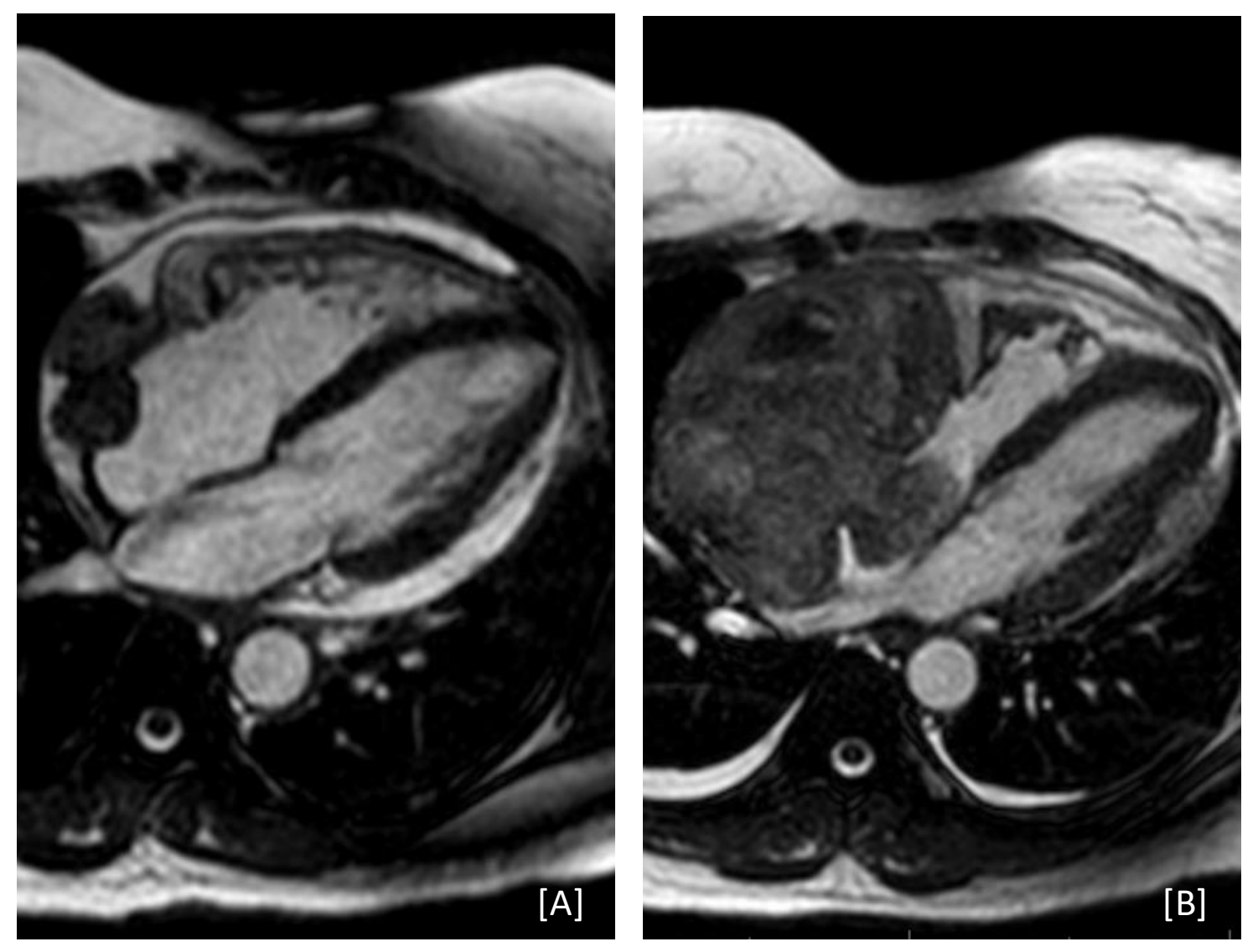
Case Presentation: A 53-year-old female with history of two recent admissions for idiopathic pericarditis presented with several days of increasing chest pain, dyspnea, and lightheadedness. During her first admission three months prior, she underwent urgent pericardiocentesis with pericardial drain placement for early cardiac tamponade. Fluid cytology results were unremarkable. Cardiac computed tomography demonstrated a focal, lobulated contour change of the right atrium initially attributed to post-operative change. Transthoracic echocardiography and cardiac magnetic resonance imaging (MRI) demonstrated a 2.4 x 2.0cm well-circumscribed, lobulated mass thought to be thrombus or hematoma after discussion with cardiology and cardiothoracic surgery. She was discharged with ibuprofen and colchicine with plans to repeat imaging in several weeks. She was briefly readmitted four days later with similar symptoms found to have atrial flutter with rapid ventricular response. She responded well to amiodarone and discharged on a taper, which she finished by the time of current admission.On presentation, she was hemodynamically stable with labs notable for leukocytosis (14.3 x 10^9/L white blood cells) and elevated C-reactive protein (18 mg/L, decreased from a peak of 128 mg/L in her first admission). Repeat cardiac MRI discovered significant growth of the mass to 11.6 x 7.7cm, with a contiguous portion projecting into the right atrium. A separate mass was also found on the left atrial wall measuring 2.0 x 2.9cm with evidence of vascularity. Biopsy of the mass confirmed high grade angiosarcoma. Due to high surgical risk, resection was not undertaken and initial neoadjuvant chemotherapy was recommended instead. Chemotherapy with gemcitabine and docetaxel was initiated several days after discharge. However, the tumor continued to progress through chemotherapy and metastasized to her right femur 3.5 months after initial presentation. Unfortunately, she expired two months later.
Discussion: Primary cardiac angiosarcoma is a rare and aggressive malignancy most frequently affecting those under 65 years old (1). It most frequently presents as dyspnea, but also can manifest as recurrent pericarditis as our case above (2–4). Such patients are often admitted to hospital medicine services and are reliant on our accurate diagnostic work up. Early surgical resection offers the best chance of long-term survival, though median survival rates remain around 20 months (5, 6).Pericardial fluid cytology is unreliable, with malignant cells rarely found even with invasive tumors (3, 7). Comparatively, transthoracic and transesophageal echocardiography are estimated to be ~90% sensitive for cardiac masses, though in our case, the patient’s tumor was not discovered by initial transthoracic echocardiography (1, 8, 9). In a direct comparison, cardiac MRI was more sensitive than echocardiography for cardiac masses (10).
Conclusions: Cardiac angiosarcoma is a rare disease but should be on the differential for a patient with recurrent pericarditis despite optimal medical management. Repeat imaging should be considered. Prompt diagnosis and surgical management offers patients the greatest potential for survival.