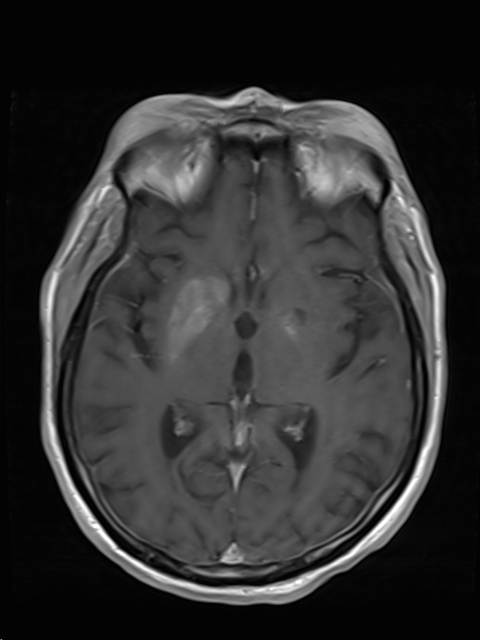
Case Presentation: A 62-year-old female with past medical history of poorly controlled Type 2 diabetes mellitus and hypertension, presented to the emergency department with complaints of altered mental status. Her physical exam was positive for tenderness over the lower abdominal area. Initial lab work was notable for leucocytosis [WBC of 18.9 bil/L (normal 3.3- 10.7 bil/L) and neutrophils 15.2 bil/L (normal 1.6-7.2 bil/L)]. Her blood glucose was 531 mg/dl (Normal 71-139 mg/dl). Beta hydroxybutyric acid level was 1.02 mmol/L (Normal 0.02- 0.27 mmol/L), Anion gap of 8 (normal 5-17), bicarbonate of 16 mmol/L (normal 20- 29 mmol/L, Blood osmolality of 311 mOsmal/kg (normal 275-295 mOsmol/kg). Her glycated Hemoglobin was 16.3 % (Normal 4 –5.6%). Due to decline in mentation, Stroke Team was activated. NIHSS score was 17. Head Computed Tomography (CT) scan revealed hyperattenuation suggestive of hemorrhage in the right basal ganglia (2.4 cm) and calcification in the bilateral basal ganglia without midline shift. Additionally, CT scan of the abdomen revealed an intra-pelvic abscess in the posterior vagina. She was started on antibiotics and taken for surgical debridement. Conservative approach was pursued for the hemorrhagic stroke. MRI of the brain, done two days later, demonstrated T1 signal hyperintensity involving bilateral lentiform nuclei, greater on the right. This area corresponded to the area of hyperdensity seen in the prior Head CT. A subsequent head CT done 3 weeks later showed interval resolution of previously seen hyperdensities. Eventually, with control of hyperglycemia and treatment of pelvic abscess, her mental status returned back to baseline.
Discussion: Abnormal variations in plasma glucose levels are not uncommon. The presentation is nonspecific and can mimic stroke due to neurological deterioration. This is usually due to cerebral edema. Hyperglycemia causes endothelial dysfunction and increased oxidative stress in ischemic brain tissue. Underlying comorbidities such as diabetes mellitus increases the risk of intracerebral hemorrhage. It can present with myriad imaging findings. As seen in our case, the NIHSS stroke scale was high and initial head CT was suggestive of hemorrhagic stroke. Fortunately, MRI was done prior to surgical intervention for the presumed intraparenchymal bleed. MRI findings of T1 hyperdensities are seen in hepatocerebral degeneration, hyperglycemia, or disorders of calcium and phosphate metabolism. In our patient, this was attributable to hyperglycemia. The pathogenesis of such imaging findings is controversial and is further compounded by variable histopathology results from different studies. Focal hemorrhage and calcification were initially proposed but these are not consistent features on histopathology. Interval resolution of findings on follow-up imaging also do not favor hemorrhage or calcification as a common finding.
Conclusions: Mental confusion and coma are common occurrences in hospital. Imaging can suggest the diagnosis in unsuspected cases. The management approach of intraparenchymal hemorrhage and cerebral edema due to hyperglycemia are distinct. Timely recognition can be crucial in avoiding neurosurgical intervention and providing accurate care. Therefore, clinicians should be aware of both common and atypical neuroimaging findings of hyperglycemia and the potential mimic between pseudo-intraparenchymal bleed and cerebral edema.