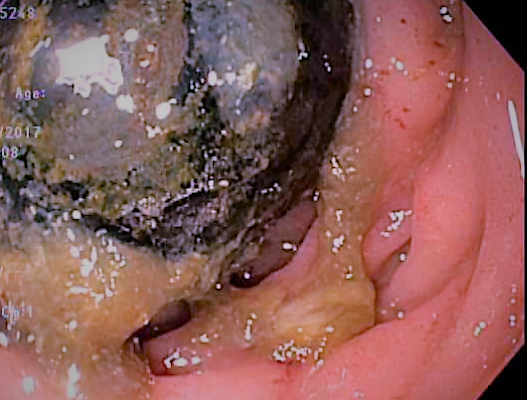
Case Presentation: A 74-year-old woman presents to the ED with acute on chronic right upper quadrant pain that awoke her from a dead sleep. She reported struggling with intermittent abdominal pain, nausea, and vomiting over the past several months, but not previously this severe. Patient denied fevers or chills. Labs were remarkable for leukocytosis, transaminitis, and elevated lipase. A CT abdomen revealed diffuse pneumobilia in the bile and hepatic duct as well as gallbladder. No common bile duct dilatation was visualized. The CT scan was followed by MRCP, which demonstrated a cholecysto-duodenal fistula with a 3.0cm gallstone at the level of the fistula, and another 2.3cm gallstone in an ileal loop. EGD revealed a 1.5cm obstructing biliary stone in the 2nd portion of the duodenum consistent with Bouveret’s syndrome. The stone was removed via basket retrieval during endoscopy. ERCP was performed without visualization of the fistula. Multiple stones were swept from the common bile duct, and a stent was placed given MRCP findings. She recovered well and was discharged the following day.
Discussion: Gallstone ileus is an uncommon complication of cholelithiasis as well as an uncommon etiology of mechanical small bowel obstruction. It is most commonly seen in elderly females with a history of hypertension and diabetes, and is the cause of 25% of mechanical small bowel obstructions in patients older than 65 years old. The typical etiology for gallstone ileus is reoccurring cholecystitis secondary to cholelithiasis with subsequent cystic duct obstruction. The repeated inflammation and subsequent adhesions results in a cholecysto-enteric fistula, which was the likely modality of entry for our patient’s stone. Management of gallstone ileus typically requires surgical management. However, in Bouveret’s syndrome the stone establishes a fistula and migrates to the duodenum, and less invasive removal is often attempted first via endoscopy with or without lithotripsy. CT scan is not always diagnostic of Bouveret’s or gallstone ileus, as once stones enter the gut they have similar appearance to calcified stool. Pneumobilia is a common finding; however, and when present should prompt further diagnostic imaging (MRCP).
Conclusions: • Pneumobilia on CT with clinical signs of mechanical obstruction should raise suspicion for a cholecysto-enteric fistula, which is best visualized on MRCP.• Bouveret’s is an uncommon cause of mechanical bowel obstruction, but should be considered in elderly females with a history of cholelithiasis, hypertension, and diabetes who present with obstructive symptoms.