Background: Hospitalization is costly, associated with the potential for adverse medical events and may have deleterious health effects. Hospitalist physicians are uniquely positioned to help patients avoid unnecessary hospitalizations. Our attending-only hospitalist practice in a tertiary academic center admits approximately 350 patients monthly, the majority of which are referred through the emergency department (ED). Our group has the option of providing consultation and discharging patients from the ED if appropriate. Characteristics and outcomes for patients discharged from EDs by hospitalist physicians have not yet been described.
Methods: We performed an uncontrolled retrospective observational study of patients discharged from the ED after referral for hospitalist admission. Patients were identified via Current Procedural Terminology (CPT) billing codes for consultation performed in the ED linked to physicians in our hospitalist group. The study period was April 2011 to April 2014. We recorded basic demographics and International Classification of Disease, version 9 (ICD9) primary diagnosis codes. Similar codes (i.e., chest pain NOS and musculoskeletal chest pain) were grouped together. Primary outcomes included return to the ED within 30 days and hospitalization within 30 days. Rates were calculated using a generalized linear mixed-effects model (GLMM) to account for the non-independence of the data, along with Wald confidence intervals.
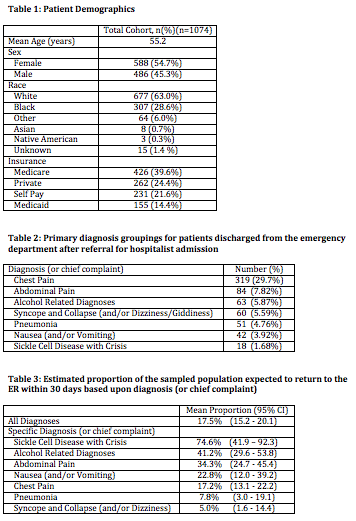
Results: We identified 1074 patients. Mean age was 55.2 years and 54.7% were female (Table 1). Chest pain was the most common diagnosis (29.7%, Table 2). For the entire cohort, the rate of returning to the ED within 30 days was 17.5% (CI 15.2-20.1, Table 3). The rate of hospitalization within 30 days was 6.0% (CI 4.7-7.6). The three diagnosis groups with the highest rates of return to the ED were sickle cell disease with crisis (74.6%, CI 41.9 – 92.3), alcohol related diagnoses (41.2%, CI 29.6 – 53.8), and abdominal pain (34.3%, CI 24.7 – 45.4). Patients with chest pain had a rate of return to the ED similar to that of the entire cohort (17.2%, CI 13.1 – 22.2).
Conclusions: The large majority of patients discharged from the ED after referral for hospitalist admission did not return to the ED within 30 days and the risk of hospitalization within 30 days was low. Almost one-third of the discharged patients were evaluated for chest pain. Patients with sickle cell disease, alcohol related diagnoses and abdominal pain had higher rates of ED revisits when compared with the entire cohort, though relatively few patients in our study had these diagnoses. These results have significant implications for hospitals and physicians seeking to improve patient care by avoiding unnecessary hospitalizations.