Background:
General wards are high-risk clinical areas, but frontline staff face operational challenges not prioritized in national safety initiatives. Team reporting may identify important risks to patient care, although its impact as a safety strategy is unknown. We developed HEADS-UP (Hospital Event Analysis Describing Significant Unanticipated Problems), a system for prospective clinical team surveillance (PCTS). It combines structured daily interdisciplinary briefings to capture safety threats with facilitated escalation to senior clinicians and managers. In this cluster controlled stepped wedge trial, we evaluate PCTS’ impact on patient outcomes, unit climate, and incident reporting.
Methods:
HEADS-UP was sequentially introduced to 6 medical wards between 2013-2015 in a UK community hospital, alongside the existing incident reporting system. Ward teams underwent initial training and then led their own briefings. Feedback was delivered regularly to participating teams and managers.
Implementation was assessed with completed briefing proformas and field notes. Safety and teamwork attitudes were evaluated with the Safety Attitudes Questionnaire. Patients were eligible if they had not undergone multiple intra-hospital transfers, and were not discharged to a new nursing facility. Generalized estimating equations accounted for clustering, temporal trends, patient age, Charlson score, ward admissions, and palliative care status. We defined excess length of stay (eLOS) as an admission lasting 24hrs longer than the local average for the patient’s Healthcare Resource Groups (standard codes used in the UK to categorize diagnoses and treatments).
Results:
We analysed 11,225 patients, 852 HEADS-UP briefings, 93 surveys and 2073 incident reports over a 19-month period. HEADS-UP was performed on 77% of working days/month, documenting 83 issues/month. 70% of participants agreed they reported concerns differently as a result of the program. Safety and teamwork scores improved (p=0.008 and p<0.001 respectively).
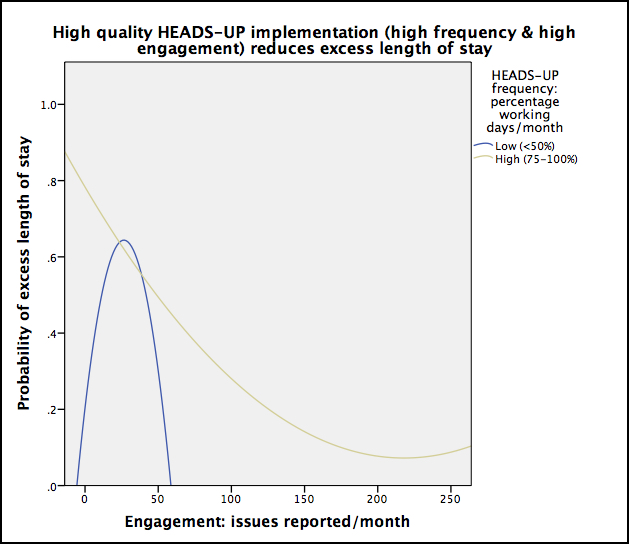
High quality HEADS-UP – more frequent briefings with better documentation – significantly reduced eLOS (p=0.039; OR 0.82, 95% CI 0.72-0.93 for high vs low frequency briefings; see Figure). High quality HEADS-UP also increased meaningful incident reports (p=0.002), incident reporting by medical staff (p=0.025), and patient transfers to ICU (p=0.016). HEADS-UP generated $37,600 in internal investment, and in November 2014 was commended as outstanding practice by the UK’s national quality inspectorate, the Care Quality Commission.
Conclusions: High quality PCTS, using the HEADS-UP structured briefing and facilitated escalation process, improved staff attitudes, incident reporting and patient outcomes. PCTS may be a valuable adjunct to existing safety strategies.