Background: Central line-associated blood stream infections (CLABSIs) are a substantial source of morbidity and mortality. A previous meta-analysis of 1,976 CLABSI cases showed an odds ratio for in-hospital death of 2.75 (CI 1.86-4.07).[1] CLABSIs have also been associated with higher hospital costs and longer length of stay (LOS).[2]
Methods: Data was collected from all CLABSI cases attributed to Department of Medicine at a large academic center over 8 months. The type of central line and indication was examined. Data was also collected on adherence to best practices for CLABSI prevention, including consistent chlorhexidine gluconate (CHG) bathing and conversion of IV medications to enteral formulation when possible. The analysis also looked into patient characteristics to elucidate potential risk factors for CLABSI: admission from nursing facility, LOS, overall mortality, pressure injury, and use of parenteral nutrition (TPN). Descriptive statistics were calculated in Microsoft Excel.
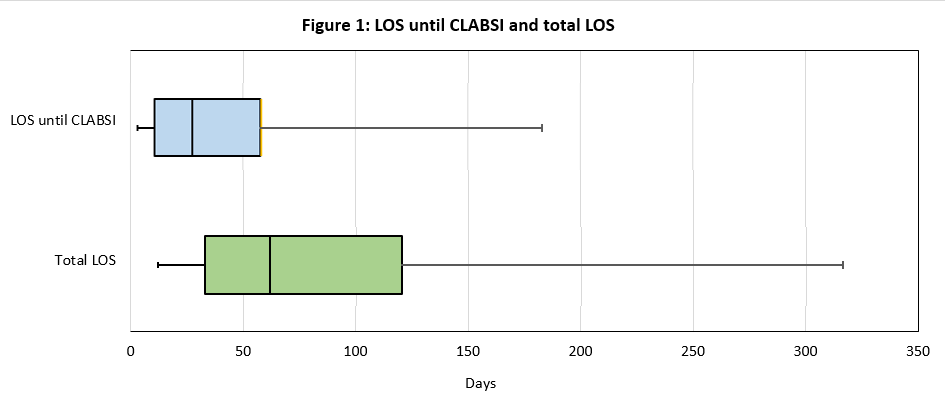
Results: There were 24 CLABSI cases in total in the Department of Medicine. The most common type of central line was tunneled dialysis catheter (n=10, 42%), followed by peripherally inserted central catheter (n=6, 25%), non-tunneled catheter (n=4, 17%), tunneled non-dialysis catheter (n=3, 13%), and subcutaneous port (n=1, 4%). Among patients who developed CLABSI, there was adherence to the institutional central line care bundle, with 100% receiving CHG bathing in the 7 days preceding the line infection and 23/24 patients receiving an IV medication that could not have been administered enterally. Patients presented from a long-term care facility in 42% of cases (n=10). The median LOS was 62 days (IQR 32.75 to 120.25). The median LOS until the time of CLABSI was 27.5 days (IQR 10.5 to 57.75) [Figure 1]. Total parenteral nutrition (TPN) was being administered in 42% of cases (n=10). In 71% of cases (n=17), the patients had a previous infection during the hospitalization. Wound/pressure injury was present in 58% (n=14). Hospice or comfort care had been recommended in 38% of cases (n=9). Patient mortality was 25% (n=6).
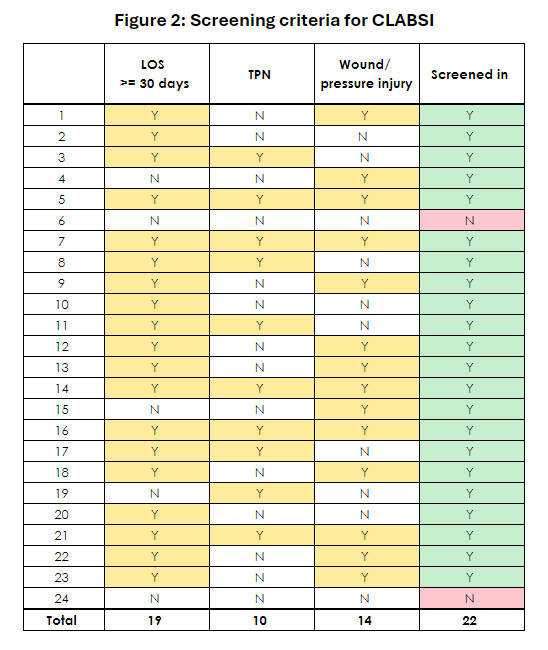
Conclusions: An analysis of CLABSIs at our institution on the Medicine service demonstrated that line infections occurred among both temporary and tunneled catheters. A CLABSI reduction bundle was in place before the time period studied, which included central line documentation, physician and nurse training, de-escalation of unnecessary lines, converting IV medication to PO, routine dressing care, and CHG bathing. Despite adherence to this bundle, there were still 24 CLABSI cases over 8 months, suggesting that these patients may have additional risk factors to address in order to prevent CLABSIs. Our analysis showed that this population of patients with CLABSI often presented from facilities and had unusually long hospital admissions. A majority of patients had a previous infection during the hospitalization, many required parenteral nutrition, and many had pressure injuries. TPN[3] and LOS[4] have both been identified as risk factors for CLABSI. To our knowledge, the presence of wounds/pressure injuries has not been reported as a risk factor, and represents an area of potential study and intervention. These results may allow us to identify patients at high risk of CLABSI. Screening patients with wounds/pressure injuries, TPN, or prolonged LOS would have identified over 91% cases of CLABSI in this series [Figure 2]. We plan to implement targeted interventions to reduce CLABSI rates in these high-risk patients.