Background: Low-value care in the form of overuse of inpatient diagnostic testing is an important driver of high healthcare costs. Financial incentives are known to impact physician behavior and may be a driver of inpatient diagnostic overuse. However, the association between hospital payer mix (which likely impacts the financial incentives for ordering diagnostic tests) and the volume of diagnostic testing overuse at hospitals has not been well characterized.
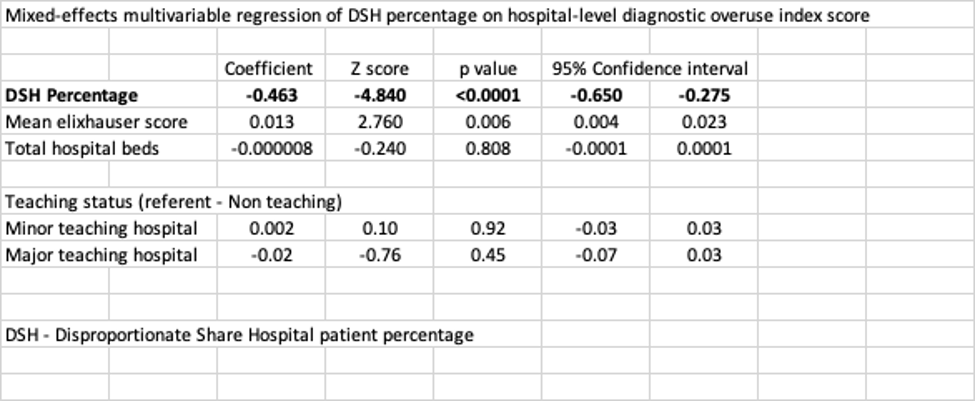
Methods: We constructed a simple hospital-level diagnostic overuse index to characterize levels of diagnostic testing (manuscript describing its development and validation is currently in press at the Journal of Hospital Medicine). Index construction employed a derivation-validation strategy, utilizing hospital data from seven states in the State Inpatient Database of HCUP. Our overuse index utilizes the concept that high rates of non-diagnostic testing paired with non-specific primary discharge diagnoses are likely associated with high levels of low-value testing. It is comprised of five metrics with good temporal stability and internal consistency, and it correlates with five of six prespecified external validation measures (hospital service area-level Dartmouth Atlas metrics and county-level Medicare cost metrics). Index values range from 0.057 to 0.986 for the 620 hospitals in our dataset with high values associated with higher levels of diagnostic overuse.To characterize the relationship between payer mix and diagnostic overuse, we utilized the Medicare Disproportionate Share (DSH) patient percentage, which CMS uses to estimate the fraction of low-income patients at a given hospital (larger fraction is associated with more low-income patients), as a proxy for payer mix. We employed a mixed-effects multivariable regression model to characterize the relationship between the index value and DSH percentage of a hospital controlling for teaching status, mean Elixhauser mortality score, hospital size (by number of beds), and state random effects.
Results: We found a strong negative correlation between DSH percentage and our overuse index (-0.46, 95% confidence interval: -0.65 to -0.28), suggesting that hospitals with a better payer mix (lower DSH percentage) are more likely to have high rates of low-value diagnostic testing (Table).
Conclusions: We developed a hospital-level index to help characterize hospitals on a spectrum of diagnostic overuse. While financial incentives are widely known to influence physician behavior, we are not aware of empirical evidence elucidating the relationship between hospital payer mix and diagnostic overuse. Hospitals with a payer mix of more commercially insured patients and fewer Medicaid patients are more likely to benefit financially from a culture and incentives that encourage low-value diagnostic tests. Future studies should attempt to further characterize this relationship using other measures of payer mix and using statistical techniques that can test for a causal relationship. As this relationship is better understood, efforts should be made to adjust financial incentives to reward value over volume.