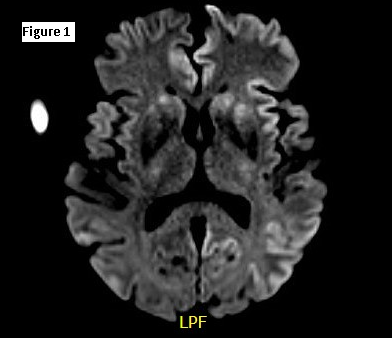
Case Presentation: Case Presentation: A 75-year-old female with a history of chronic lymphocytic leukemia, hypertension, coronary artery disease and chronic kidney disease presented with confusion that progressed to mutism, apraxia, right sided weakness and spasticity within 3 weeks. On exam, she was drowsy but arousable to voice, inconsistently following simple commands and mute. The right upper and lower extremities exhibited spastic hemiparesis with dystonic posturing and intermittent myoclonic movement. Labs revealed lymphocytic leukocytosis with smudge cells on peripheral smear. The following tests were negative or unremarkable: CT head, HIV screen, vitamin B12, folate, thyroid studies, urine drug screen, blood and urine cultures. CSF analysis showed no pleocytosis, and negative infectious workup (HSV PCR, cryptococcal Ag, VZV IgG VDRL, culture for bacteria and fungus), flow cytometry, neurosensory paraneoplastic panel and Tourtellotte analysis. CJD panel showed positive real time quaking induced conversion (RT QUIC), tau protein and 14-3-3 protein. EEG displayed sharply contoured periodic pattern mostly bifrontal. Brain MRI showed cortical ribboning, hyper intense signal in the cortical gyri on diffusion weighted imaging, and restricted diffusion in bilateral basal ganglia concerning for CJD (fig 1). Her neurological condition continued to decline, and she died within a month of presentation.
Discussion: Discussion: Creudtzfelt-Jacob disease (CJD) is the most common type of prion disease and the vast majority are sporadic (85-95%), with only 1% being infectious. Prion disease has been transmitted to humans through dietary practices and iatrogenic exposures. Rapidly progressive mental deterioration and myoclonus are characteristic signs. Brain biopsy is the gold standard for definitive diagnosis. Cases are universally fatal as no effective treatment exists, with death occurring within 1 year.
Conclusions: Conclusion: In sporadic CJD, the cortical ribbon sign is the most striking feature. Elevated CSF levels of 14-3-3 are specific for CJD. Although rare, clinicians should be aware of prion diseases and should be considered in the differential of any patient presenting with rapidly progressive neurocognitive decline.