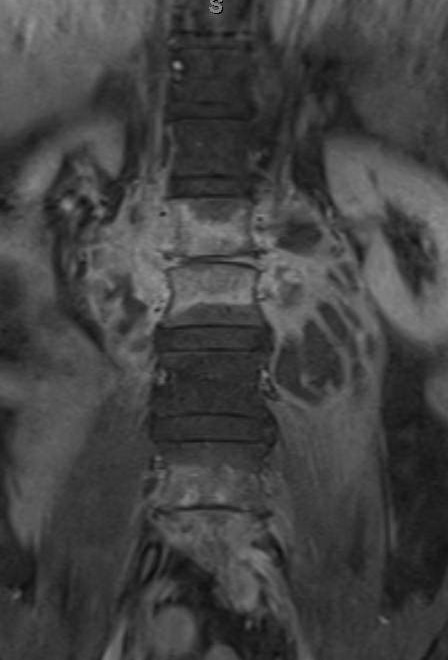
Case Presentation: A 62-year-old man presented with six months of progressive lower back pain. He noticed weight loss, sweats, and subjective fevers, but denied neurological symptoms or a other complaints. Patient lives in Texas, but travels to Mexico during winter. He denied tobacco abuse, intravenous drug use, incarceration or animal exposure. He reported eating unpasteurized cheese one year ago in Cuba and Mexico. Physical examination was positive for mild lumbar vertebral tenderness. Labs included an erythrocyte sedimentation rate of 64 mm/h and C-reactive protein of 4.4 mg /dL. White blood count was normal. Magnetic Resonance Imaging (MRI) of the lumbar spine showed infective lumbar spondylitis at L1-L2 and L4-L5 with extensive bilateral psoas abscesses. Blood and abscess aspirate cultures were obtained, and the patient was started on anti-tuberculosis medications given the classic MRI features of for tuberculosis. Abscess aspirate grew Brucella melitensis and anti-tuberculosis medications were changed to gentamycin and doxycycline
Discussion: Back pain is a common symptom encountered by internists and the differential diagnosis is broad. But it can be more concerning when other symptoms are present and in certain patients like: fever, chills, weight loss, night sweats, urinary incontinence, history of cancer or immune compromised patients… While brucellosis is one of the most common zoonotic diseases worldwide, in the United States human brucellosis is rare. Brucellae are transmitted to humans by direct contact with infected animals or consumption of unpasteurized dairy products. Brucellosis may present as a subclinical illness, an acute disease with general manifestations or as a localized disease. Osteoarticular involvement is one of the most common complications. This may present as arthritis, sacroiliitis or spondylitis.
This case describes a patient with progressive back pain who was found to have lumbar spondylitis and bilateral psoas abscesses with features typical for tuberculous spondylitis. However, the culture grew Brucella melitensis. The patient did not improve despite two weeks of therapy. Abscesses were drained, and gentamycin was changed to rifampin. Afterwards, the patient‘s back pain improved and both doxycycline and rifampin were continued for four months after abscesses drainage.
Conclusions: Brucellosis is rare in the United States and thus often overlooked in the differential diagnosis of back pain. It requires a high index of suspicion, which can result in early diagnosis and predictably favorable results to treatment.