Background: Among the challenges clinicians face when performing cardiopulmonary resuscitation (CPR) are difficult decisions regarding duration of resuscitative efforts, which may be informed by perceived prognosis as well as patient and family values and directives. There is a dearth of information on clinicians’ attitudes in these scenarios. Our aim was to determine which factors most influence the duration of CPR provided and to describe clinicians’ feelings and attitudes towards the resuscitative efforts. By elucidating these we hoped to more fully understand clinicians’ approaches to decision-making during these challenging situations.
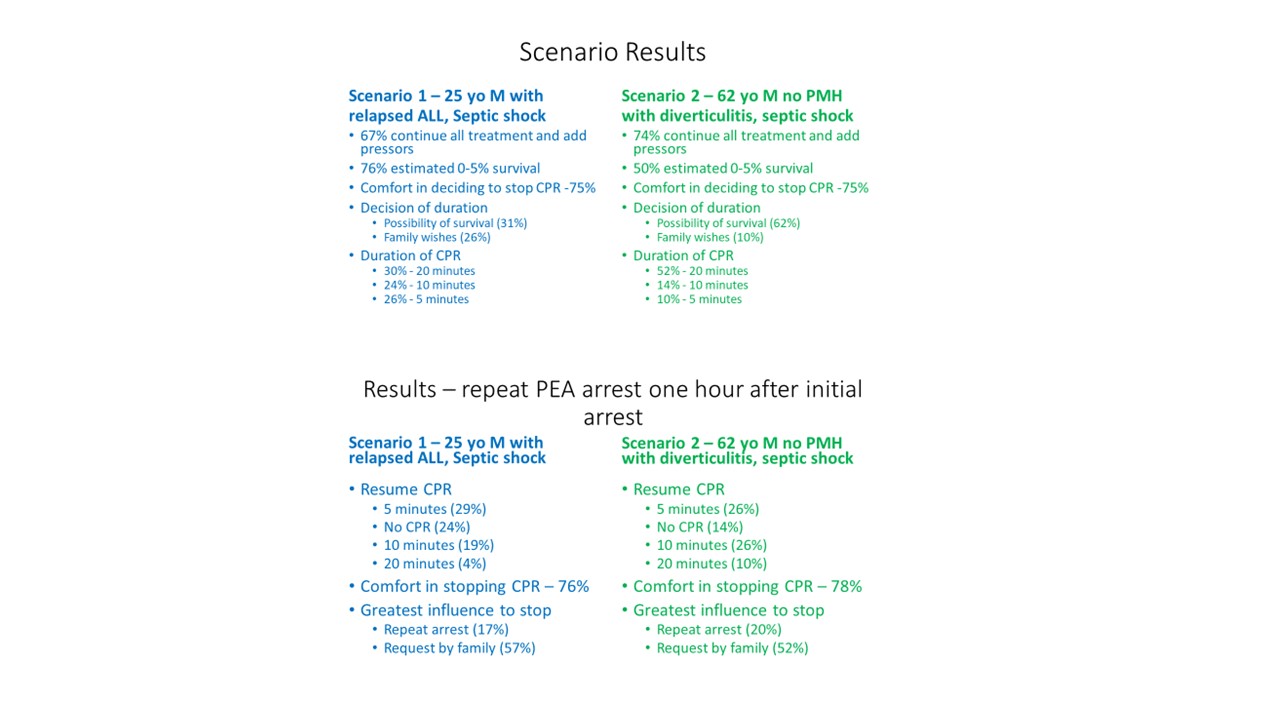
Methods: Initially we conducted a series of focus groups, consisting of hospitalists and intensivists to determine elements to be included in the survey. Based on these we created a survey that was then disseminated across two institutions to internal medicine house staff, hospitalists, as well as ICU staff including nursing, fellows, and physicians from December 2018 through September 2019. The survey included demographic information and two clinical vignettes of patients with pulseless electrical activity (PEA) arrests, followed by a series of questions that were identical in the two scenarios. Vignette 1 involved a 25 year-old patient with acute lymphoblastic leukemia with relapsed disease and septic shock, and Vignette 2 described a 62 year-old patient with no significant past medical history with septic shock from diverticulitis. Both vignettes also involved scenarios of re-arrest after the initial resuscitation.
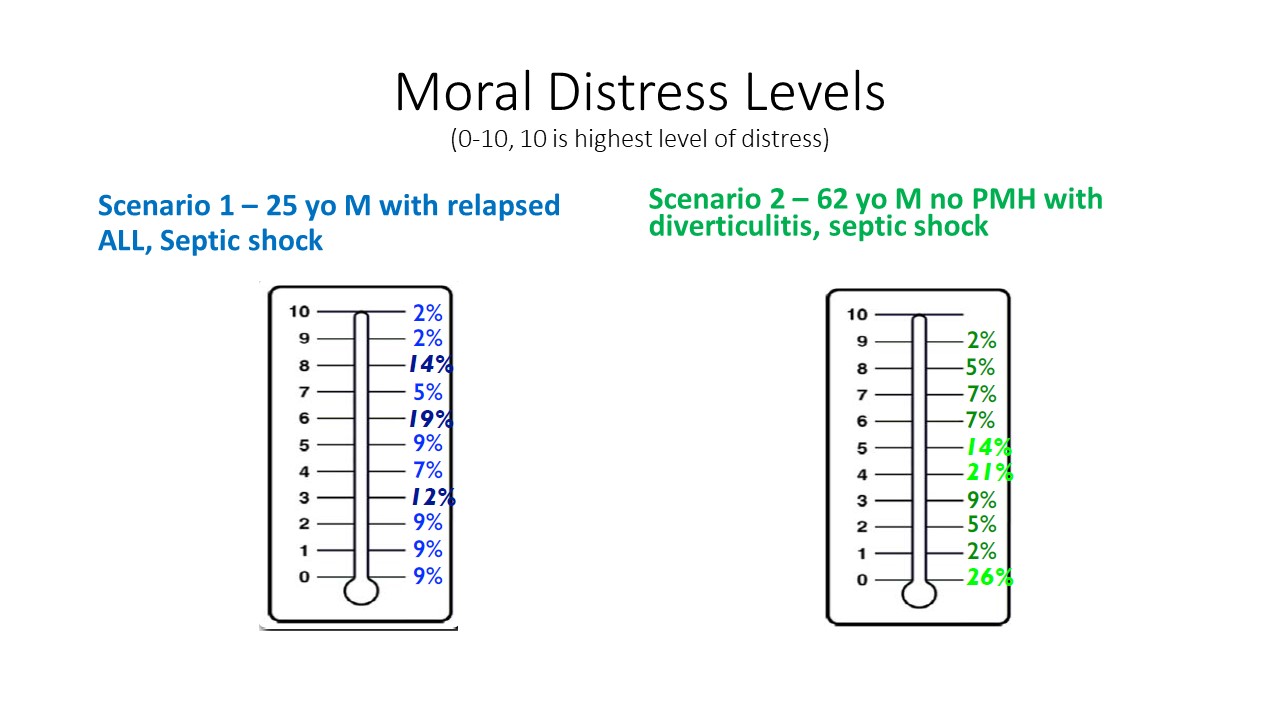
Results: We received 266 responses. Over 90% of clinicians were full-time employees and 60% were women. Over 70% of respondents had participated directly in more than 20 medical codes. In response to Vignette 1, 30% of clinicians would conduct CPR for 20 minutes, whereas in Vignette 2, 52% would continue CPR for this length of time. In Vignette 1, only 10% of those surveyed felt the patient had a 10% chance of surviving until discharge, whereas in Vignette 2, 30% felt this to be the case. In Vignette 1, family wishes (26%) along with possibility of survival (30%) primarily informed respondents’ explanation for the duration of CPR. In Vignette 2, this decision was principally informed by possibility of survival (62%). Clinicians responded similarly regarding duration of CPR during subsequent cardiac arrests for both cases. Respondents had more perceived moral distress with performing CPR in Vignette 1 compared to Vignette 2, however they described similar comfort level with determining duration of CPR in both vignettes, 75% and 79%, respectively. Family request guided the decision to stop CPR in over 50% of respondents in both scenarios. 82% of free-text comments referenced medical “futility,” but most of these also reflected that ultimately family and patient wishes guide treatment decisions in these situations.
Conclusions: Our survey data show that perceived poor overall prognosis is associated with clinicians’ decision to limit the duration of CPR and is also associated with their increased moral distress while performing CPR. Despite this distress, clinicians do feel comfortable determining the duration of CPR in these circumstances. Interestingly, no clear consensus emerged regarding the influence of family wishes on duration of CPR. Our results help illustrate how clinicians make challenging life-and-death medical decisions and could inform conversations with clinicians as well as with patients and their families regarding these scenarios.