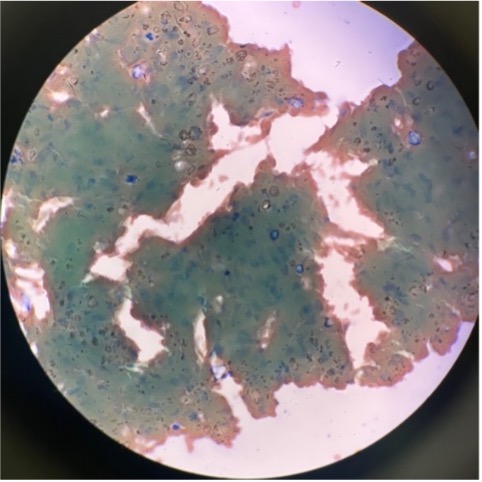
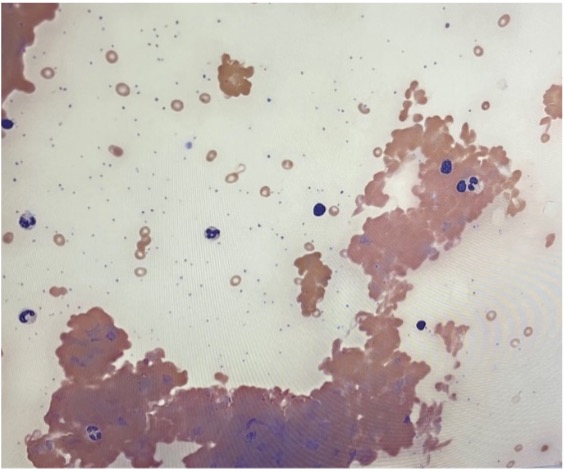
Case Presentation: A 72-year-old woman with hypothyroidism and osteoporosis presented with fevers, dysuria, and jaundice. Ten days earlier, she was treated for a urinary tract infection with ciprofloxacin. She reported intermittent fevers, persistent dysuria, and progressive yellowing of the skin over several months. On admission, she was hemodynamically stable and appeared pale, without icterus. Cardiopulmonary and abdominal exams revealed a soft systolic murmur and an abdominal bruit. Laboratory evaluation showed severe macrocytic anemia (Hb 4.4 g/dL, Hct 12.2%), reticulocytosis (18.6%), elevated LDH (1202 U/L) and total bilirubin (3.2 mg/dL), and normal iron studies with decreased TIBC. Peripheral smear demonstrated macrocytosis with marked agglutination. The direct antiglobulin test was C3-positive and IgG-negative, confirming cold agglutinin disease (CAD).She received three units of warmed packed red blood cells, targeting hemoglobin > 7 g/dL, and was discharged with outpatient hematology follow-up and instructions to avoid cold exposure.Five days later, she was readmitted with dizziness and dyspnea. She was COVID-19 positive, with hemoglobin 4.6 g/dL and bilateral deep vein thromboses. Serum protein electrophoresis revealed an IgM kappa double gammopathy (M-spike 0.7 g/dL). Bone marrow biopsy showed a low-grade B-cell lymphoproliferative disorder. She was started on rituximab therapy.
Discussion: Cold agglutinin disease (CAD) is an uncommon, complement-mediated autoimmune hemolytic anemia (AIHA) that primarily affects older adults.¹,² When no obvious infectious or autoimmune trigger is identified, hemolysis may serve as an early indicator of an underlying lymphoproliferative disorder or malignancy.²In this case, the subsequent diagnosis of a low-grade B-cell lymphoproliferative disorder underscores the importance of comprehensive hematologic evaluation. The patient’s readmission with COVID-19–associated worsening anemia and DVTs highlights the well-recognized risk of hemolytic exacerbations and thromboembolic complications during febrile or inflammatory states.³Up to 75% of patients with CAD have an underlying B-cell lymphoproliferative disorder, most commonly lymphoplasmacytic lymphoma.² Beyond malignancy, recent reports have suggested a temporal association between COVID-19 infection or vaccination and the onset of AIHA, possibly reflecting immune dysregulation or aberrant B-cell activation in predisposed individuals.⁴,⁵ In this case, SARS-CoV-2 infection likely precipitated hemolytic relapse and accelerated recognition of the underlying clonal process.Evidence on rituximab safety in patients with concurrent CAD and COVID-19 is mixed; earlier reports suggested poorer survival, while recent reviews found no increased risk.³,⁶ Careful therapy selection and monitoring remain essential.
Conclusions: The patient’s presentation with severe anemia, COVID-19 infection, and subsequent discovery of a B-cell lymphoproliferative disorder illustrates the interplay between infection, immune dysregulation, and neoplastic processes.¹,⁴ Early recognition of hemolysis, differentiation from warm AIHA, and use of warmed transfusions are critical to avoid complications.² Identification of an underlying clonal disorder guided initiation of targeted therapy with rituximab, reinforcing the importance of a comprehensive evaluation.³,⁶