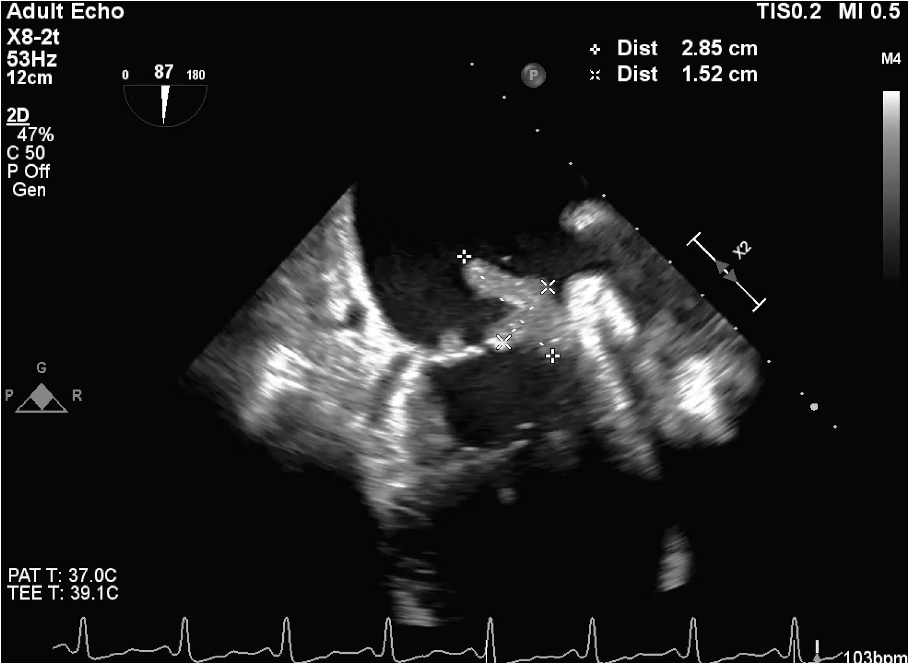
Case Presentation: 58-year-old male with history of psoriatic arthritis previously well controlled on adalimumab, presenting with 4 days of weakness, fever, joint pain, and inability to walk. After an insurance-mandated switch from adalimumab to a biosimilar, followed by an allergic reaction and a subsequent failure to authorize an alternative agent, he experienced a two-month lapse in biologic therapy. During this time, he developed a severe, painful psoriatic arthritis flare that could not be adequately controlled with topical agents. Workup revealed sequelae of sepsis along with methicillin-susceptible Staphylococcus aureus (MSSA) bacteremia, thrombocytopenia, acute kidney injury, troponinemia, and lactic acidosis. His severe flare was evidenced by diffuse psoriatic plaques on the trunk and extremities (Image 1). TTE showed no clear vegetation, though image quality was limited by body habitus. Persistent bacteremia despite appropriate antibiotics prompted a TEE, which discovered multiple independently mobile vegetations attached to both leaflets of the mitral valve, measuring up to 2.85 cm x 1.5 cm in size (Image 2). Upon discovery of the massive left-sided endocarditis, we pursued brain MRI to assess for subclinical neurological complications and found multiple foci compatible with acute infarcts via septic emboli. He was then transferred for valve repair and further management.
Discussion: MSSA native valve infectious endocarditis (NVIE) is a serious infection of the heart valves, often arising from bacteremia. This can be a life-threatening development in patients with severe psoriasis, where damaged skin serves as a source of infection. Additionally, MSSA NVIE is highly aggressive, with friable vegetations leading to CNS embolic events up to 65% of the time, and mortality rates of 25-40%.¹ Notably, this patient lacked typical risk factors for endocarditis — no history of intravenous drug use, valvular disease, implanted cardiac devices, or dental infection. Rather, it was a gap in insurance coverage that likely led to his extensive psoriatic flare and skin barrier breakdown, producing a source for MSSA bacteremia that progressed to significant endocarditis and subclinical CNS emboli. He is part of the 40% of Staphylococcus aureus endocarditis cases that occur in patients with no known predisposing conditions, emphasizing the relevance of often overlooked social risk factors.² This case demonstrates the importance of thorough evaluation to detect clinically silent complications of bacteremia, and more broadly, how insurance-mandated changes in therapy and delays in approval can destabilize well-controlled chronic disease, leading to preventable clinical risks.
Conclusions: This case illustrates a key social risk factor impacting countless patients today: challenges in insurance coverage. It highlights how insurance-related barriers to therapy can lead to devastatingly adverse patient outcomes. As healthcare costs continue to rise, the impact of the transition period between medications, or even different insurance companies, must be more closely examined. Patient advocacy for timely access to therapy is critical, as even small lapses could lead to serious complications. Additionally, we should account for these lapses in our diagnostic reasoning, as they are pertinent, legitimate causes of severe disease in vulnerable patient populations.