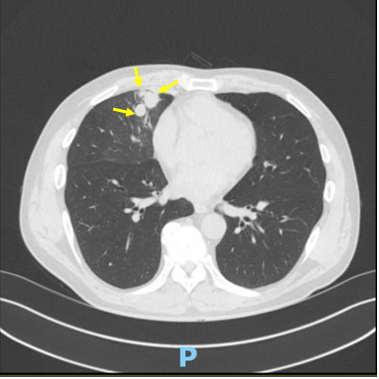
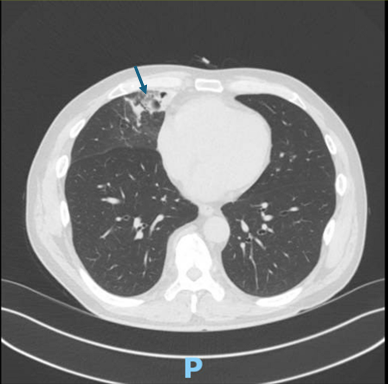
Case Presentation: A 57-year-old man with a history of coronary artery disease (status post coronary artery stenting), type 2 diabetes mellitus, hypertension, alcohol use disorder, and well controlled HIV on antiretroviral therapy (HIV viral load was undetectable; CD4 783 cells/mm³) presented with several days of mild hemoptysis. He remained afebrile, without shortness of breath or chest pain. His medications included efavirenz, emtricitabine, tenofovir disoproxil fumarate, dual antiplatelet therapy, atorvastatin and metformin. Laboratory workup was unremarkable, and a QuantiFERON-TB Gold test was negative. Chest CT revealed multiple mycetomas in the right middle lobe with surrounding ground-glass opacities and consolidation, suggestive of localized hemorrhage. He underwent elective video-assisted thoracoscopic (VATS) robotic-assisted lobectomy with mediastinal lymph node dissection and biopsy. Postoperatively, he was admitted to the ICU with a chest tube on water seal; a small apical pneumothorax was noted. Pathology revealed reactive lymphadenopathy, no acid-fast bacilli, and fungal debris in a background of bronchiectasis with acute and chronic inflammation. Fungal culture yielded Scediosporium sp. Bacterial and AFB cultures were negative. Voriconazole was initiated and antiretrovirals were changed to bictegravir, emtricitabine, tenofovir alafenamide (Biktarvy®) to avoid drug interaction. Follow-up imaging showed decreased size and improved appearance of the mycetoma. The patient recovered and is doing well.
Discussion: Fungus ball (mycetoma) is well described in immunocompetent individuals, typically forming within residual pulmonary cavities, most often due to prior tuberculosis. While rare, it has been reported in HIV-infected patients, particularly those with structural lung damage from prior pneumocystosis or necrotizing pneumonia. Our case is unique in that the patient had well-controlled HIV and preserved immunity yet developed a biopsy-proven pulmonary mycetoma. Structural lung disease, independent of immune status, may be sufficient to predispose to fungal colonization. Unlike typical HIV cases, our patient presented with significant hemoptysis, a feature more common in immunocompetent hosts. Management was complicated by drug-drug interaction between voriconazole and efavirenz-based ART, requiring a switch to Biktarvy to ensure safe and effective antifungal therapy. Surgical resection remains the definitive treatment in localized cases, especially in patients with recurrent hemoptysis.
Conclusions: This case illustrates that pulmonary mycetoma can occur in HIV-positive patients even in the absence of severe immunosuppression. Structural lung abnormalities, rather than immune status alone, appear to play a central role in predisposing to fungal colonization. Despite a preserved CD4 count, our patient developed aspergilloma, presenting with hemoptysis—a potentially serious complication. Management required careful adjustment of antiretroviral therapy to avoid drug-drug interactions with voriconazole. Surgical intervention confirmed the diagnosis and aided in symptom control. Clinicians should maintain a high index of suspicion for fungal infections in HIV patients with cavitary lung disease, regardless of immune competence. Early recognition and individualized therapy are key to successful outcomes.