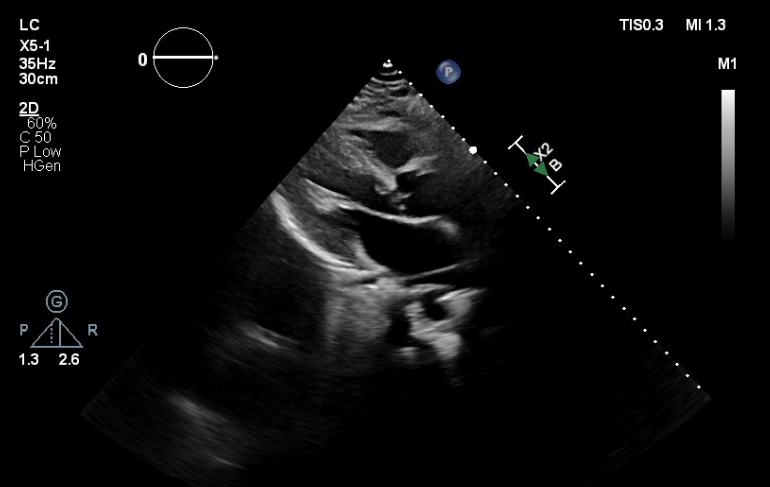
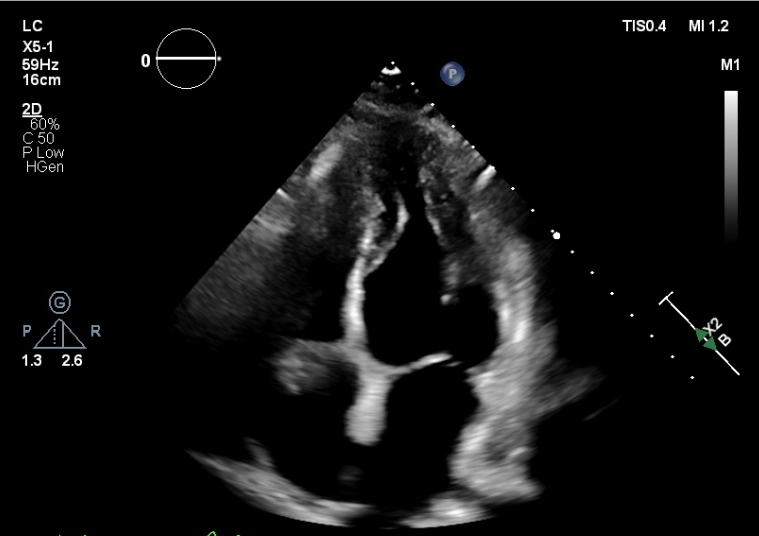
Case Presentation: A 66-year-old woman with a history of Takotsubo cardiomyopathy (2018), paroxysmal atrial fibrillation, hypertension, and dyslipidemia presented with acute abdominal pain, nausea, vomiting, diaphoresis, and hypertensive urgency (BP 202/110 mmHg). She developed hypoxic respiratory distress requiring BiPAP. Transthoracic echocardiography demonstrated preserved ejection fraction (60–65%) with basal hypokinesis and apical hypercontractility, consistent with the reverse Takotsubo variant. Coronary angiography revealed only mild non-obstructive disease. During angiography, she developed atrial flutter with rapid ventricular response, which spontaneously converted to sinus rhythm. Flecainide was discontinued due to rare case reports linking it to stress-induced cardiomyopathy. The patient improved with beta-blocker and calcium-channel–blocker therapy and was discharged with cardiology and electrophysiology follow-up.
Discussion: Recurrent Takotsubo syndrome is uncommon (~4% of cases) and the reverse variant represents only ~2% of presentations. This case is notable for recurrence after a seven-year interval and an atypical basal pattern that can mimic acute coronary syndrome or flash pulmonary edema. A hypertensive crisis with sympathetic surge likely served as the precipitating trigger. Recognition of non-classic wall-motion patterns is crucial to avoid misdiagnosis and guide appropriate management.
Conclusions: Recurrent reverse Takotsubo cardiomyopathy is rare but should be considered in patients with prior episodes presenting with acute stress, hemodynamic instability, or atypical cardiac imaging findings. Early identification and individualized long-term follow-up are essential to optimize outcomes and reduce recurrence risk.