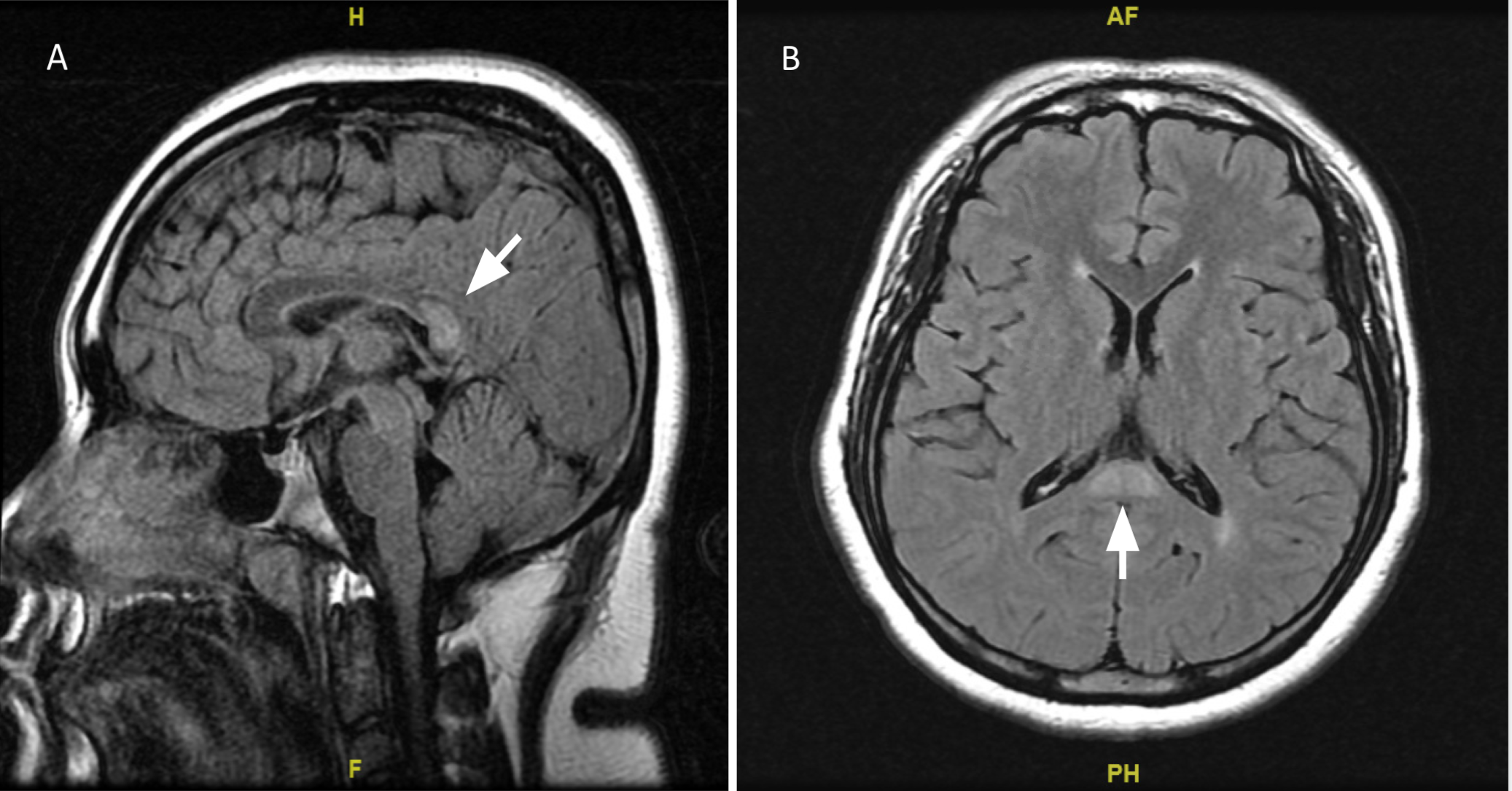
Case Presentation: A previously healthy 19 year-old female presented to the emergency room with complaints of nausea, headaches, polyuria, polydipsia and anorexia for four days. She denied urinary urgency or frequency. Her exam was unremarkable except for a flat affect and slowed speech. She was found to have hyperglycemia to 401mg/dL, elevated beta hydroxybutyrate to 2.14 mmol/L, acidosis with pH of 7.32, bicarbonate of 15.4 mEq/L, anion gap of 16 mmol/L and positive urine ketones. Treatment of diabetic ketoacidosis (DKA) was initiated with subsequent resolution. On day 2 of hospitalization, the patient reported visual hallucinations. By day 3, she became febrile to 100.6°F without increase in leukocyte count, fever workup was obtained and then started on IV ceftriaxone empirically. In addition, the patient’s headaches had not resolved with pain medication, and there was an association with new onset neck stiffness and photophobia. Her exam was unremarkable for nuchal rigidity, Brudzinski and Kernig signs. Her affect and motor response remained altered. Neurology service was consulted and a decision to utilize a less invasive approach by obtaining a brain MRI. Imaging revealed a T2 hyperintensity with restricted diffusion in the splenium suggestive of cytotoxic lesions of the corpus callosum. Later, laboratory investigations revealed positive blood cultures and she was subsequently diagnosed with E.coli bacteremia secondary to a urinary tract infection. The patient was discharged day 6 with resolution of symptoms.
Discussion: The association between mild encephalitis/encephalopathy with reversible lesions in the splenium of the corpus callosum (MERS), was first proposed in 2004 by Tada et al., and is now considered to be an acute clinico-neuroradiological syndrome secondary to drugs, malignancy, infection, and metabolic disorders. The lesions present as a solitary hyperintense mass in the splenium of the corpus callosum on MRI, that usually heals within a month. It has been shown to be more prevalent in men and in children. There is limited literature associating metabolic disturbances like diabetes ketoacidosis and E.coli bacteremia with cytotoxic lesion of the corpus callosum in the setting of mild encephalitis. The clinical symptoms of MERS are nonspecific and diverse, with the most common being fever and headaches. Digestive tract disturbances (vomiting and diarrhea), slurred speech, neck stiffness, somnolence, visual disturbances, tremor and ataxia and behavioral changes are also reported. Our patient presented with low grade fever, and neuropsychiatric symptoms including new onset headaches, somnolence, slowed speech, visual hallucinations and flat affect that could be explained by her MRI findings. This case further expands the spectrum of acute neurological complications of complicated cystitis with E.coli bacteremia and DKA, as manifested by her symptoms and imaging findings. Management of MERS is based on treating the underlying cause and symptomatic therapy. In this case, the patient responded well to glycemic control and antibiotic regimen with resolution of her neurological symptoms.
Conclusions: Alternate etiologies should be pursued when the mental status does not return to baseline. Cytotoxic lesions are rare but important to consider in the differential of altered mental status. Acquiring knowledge of this syndrome and the morphological MRI findings, is critical to establish a prompt and reliable diagnosis.