Background: Emergency Department (ED) boarding and delayed admissions contribute to overcrowding, prolonged inpatient stays, adverse clinical outcomes, and physician burnout. At our large tertiary care, Level I trauma center, hospitalists traditionally managed both inpatient rounding and new ED admissions. This dual responsibility often resulted in delayed consult-to-bed request times, care fragmentation, and workflow inefficiencies, collectively prolonging ED throughput. Recognizing the need for a sustainable, system-level intervention, we developed a dedicated “Admitting Shift” to streamline admissions and optimize patient flow.
Purpose: To improve admission efficiency, reduce length of stay (LOS), and enhance hospitalist satisfaction through a structured, dedicated “Admitting Shift” model within the hospitalist service.
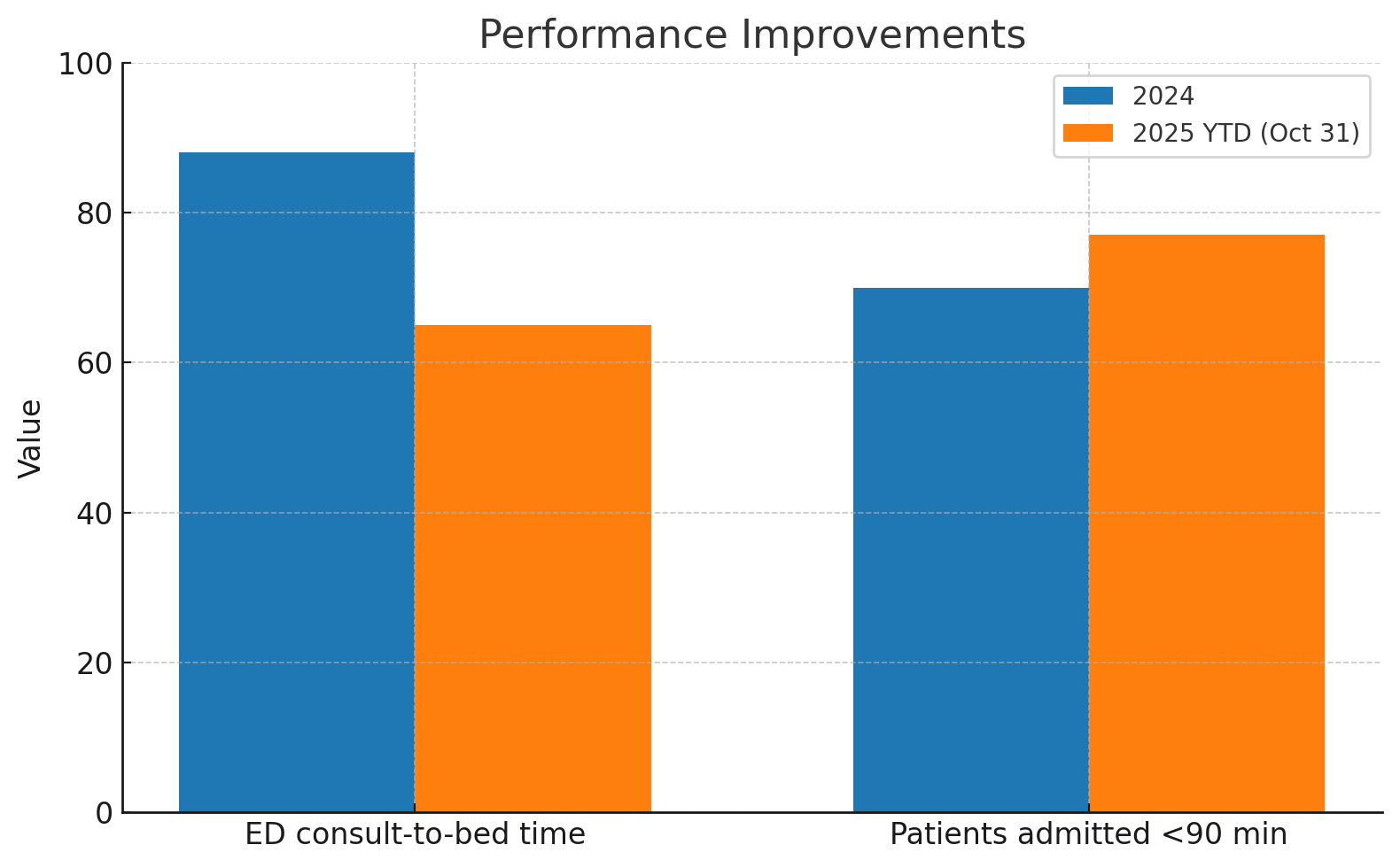
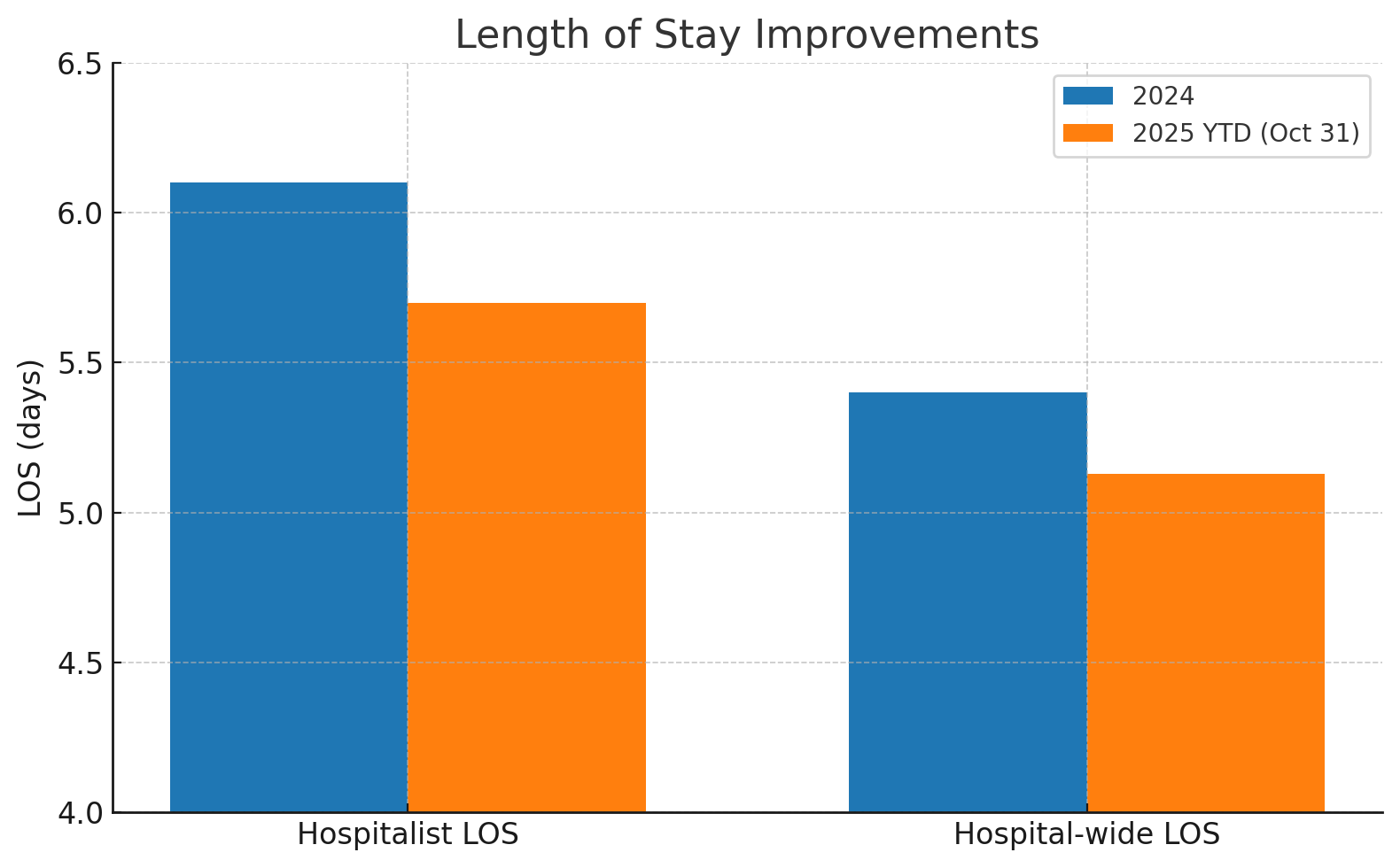
Description: In January 2025, a dedicated Admitting Shift was implemented, staffed by one physician (7 AM–7 PM) and one nurse practitioner (6 AM–6 PM) focused exclusively on ED admissions. The design emphasized transparency in workload distribution, alignment with hospital volume trends, and equitable scheduling. No new positions were created; existing shifts were restructured. Although not entirely budget-neutral, modest institutional support was provided in the form of incentives for physicians assuming Admitting Shifts, reflecting the demonstrated value and long-term sustainability of the model.Performance metrics demonstrated (2024 vs YTD through October 31, 2025):ED consult-to-bed request time: reduced from 88 → 65 minutes (26% improvement)Patients admitted within 90 minutes: increased from 70% → 77%Hospitalist LOS: improved from 6.1 → 5.7 days (6.6% reduction) across 15,264 vs 13,811 inpatient admissionsHospital-wide LOS: decreased from 5.4 → 5.13 days (5% improvement)Estimated financial impact: A 0.4-day reduction in hospitalist LOS across 13,811 inpatient admissions from 2024 to YTD October 31, 2025 (annualized to ~6,600 freed bed-days) corresponds to approximately $6.6 million in annual value, assuming a conservative $1,000 marginal value per inpatient day in a 710-bed hospital.Post-implementation survey: 96% hospitalist satisfaction, reflecting improved workflow balance, reduced interruptions during rounds, and greater role variety; ED leaders similarly reported enhanced throughput and reduced congestion during peak hours
Conclusions: The dedicated Admitting Shift improved ED throughput, reduced LOS, and enhanced hospitalist satisfaction with only modest financial investment and without additional full-time staffing. By delineating admitting and rounding responsibilities, the model minimized interruptions, improved responsiveness to ED consults, and alleviated ED crowding through continuous, dedicated coverage. This initiative demonstrates that targeted workflow redesign can produce substantial operational and financial benefits in large hospitalist programs. The Admitting Shift model provides a scalable and reproducible framework for hospitalist services seeking to improve patient flow, reduce burnout, and enhance system performance.Key Takeaway:Beyond immediate efficiency gains, this initiative showed that a thoughtfully designed, collaborative admitting model can align physician well-being, patient safety, and hospital performance, creating a durable “win-win-win” framework for system-level improvement.