Background: Central line–associated bloodstream infections (CLABSIs) are preventable yet associated with high morbidity and mortality. Literature review highlights that patients with CLABSI had higher mortality rates, readmission rates, and longer length of stay. Local institutional Vizient data showed 65% of CLABSIs occurred within 20 line-days, prompting adoption of a structured central venous access device (CVAD) removal protocol to reduce this risk.
Purpose: To assess the effect of a multidisciplinary CVAD review process on central line utilization, reinsertion rates, and CLABSI incidence during Phase 1.
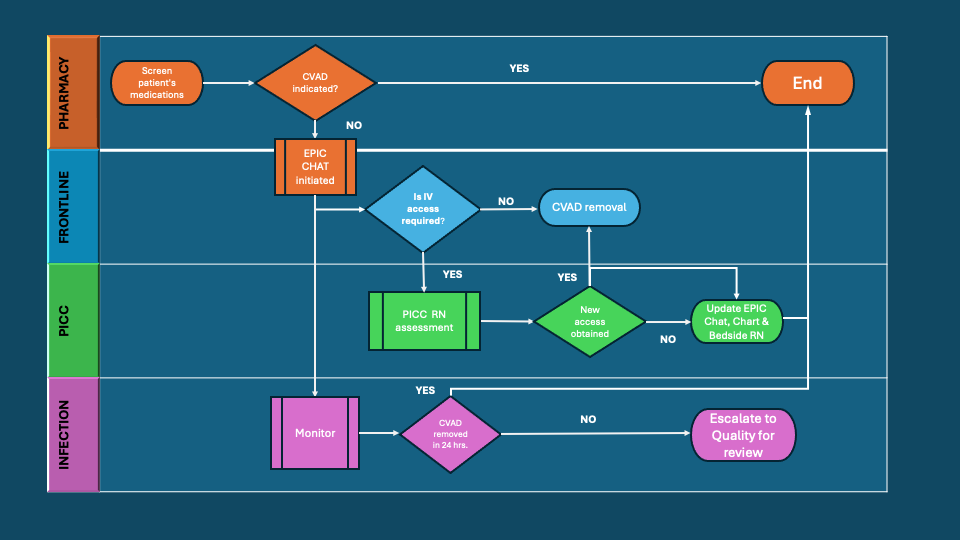
Description: A Plan-Do-Study-Act (PDSA) initiative was conducted on two medicine units. Interventions included daily reviews of CVAD necessity by a multidisciplinary team of nursing and pharmacy staff, who identified patients, assessed ongoing central line indications, and contacted the primary team via EMR chats with their recommendation to determine if removal was appropriate. Resident liaison acted as an additional contact for onsite communication. The hospital’s vascular access team was involved as needed to evaluate peripheral IV options prior to central line removal. Data collected included device type, dwell time, timing of removal, and reinsertion events. In Phase 1, 24 patients with CVADs were assessed (21 PICCs and 3 CVCs). As a result, 75 percent of CVADs were removed within 24 hours of assessment, resulting in 56 CL-free days. No CLABSIs occurred, and no CVAD reinsertions were required.
Conclusions: A structured CVAD removal protocol effectively reduced unnecessary central line days without increasing reinsertion rates or CLABSI incidence. These results support broader implementation across units to enhance patient safety and promote responsible device stewardship. By reducing unnecessary central line exposure, this project aligns with national patient safety goals and demonstrates a replicable model for improving patient outcomes, reducing infection risk, and lowering healthcare costs. The successful outcomes from Phase 1 provide strong justification for sustained organizational support and broader systemwide implementation.